Abdominal Vascular Injury
Abdominal Vascular Injury
David Ray Velez, MD
Table of Contents
Arterial Injury
Aorta Injury
- Small (< 50% Diameter): Lateral Aortorrhaphy (Primary Repair)
- Use Permanent Suture (3-0 or 4-0 Polypropylene)
- May Connect Multiple Injuries into a Single Wound if Close to Each Other
- Large (> 50% Diameter): Patch Angioplasty with PTFE Graft
- May Consider Interposition Graft if Infrarenal
- Damage Control: Shunt with a Chest Tube
Celiac Axis
- Simple: Lateral Arteriorrhaphy (Primary Repair)
- Complex: Ligate (Good Collaterals)
- Gallbladder Has Poor Collaterals and Concurrent Cholecystectomy Should Be Performed if Ligating the Hepatic Artery – High Risk for Hepatic Abscess
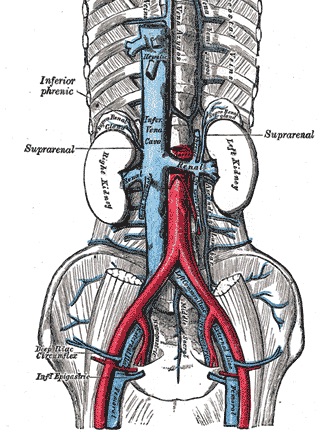
Renal Artery
- Small (< 50% Diameter): Lateral Arteriorrhaphy (Primary Repair)
- Large (> 50% Diameter): Patch Angioplasty vs Interposition Graft (Saphenous Vein or PTFE)
- Damage Control: Ligation with Nephrectomy
- First Palpate the Contralateral Kidney to Confirm Normal in Deciding the Need for Heroic Measures at Saving the Injured Kidney
Superior Mesenteric Artery (SMA)
- Fullen Classification
- Zone I – Proximal to the First Branch (Inferior Pancreaticoduodenal Artery)
- Zone II – Between the First Branch and Middle Colic Artery
- Zone III – Distal to the Middle Colic Artery
- Zone IV – Segmental Branches
- Zone I/II (Proximal to the Middle Colic):
- Stable: Primary Repair vs Bypass Graft (Saphenous Vein or PTFE)
- Bypass Grafts Should Be Made to the Distal Infrarenal Aorta (Away from the Pancreas and Potential Leak)
- Cover Grafts with Retroperitoneal Fat or Omentum to Prevent Aortoenteric Fistula
- Damage Control: Shunt vs Ligation
- Theoretically the Collaterals are Adequate to Perfuse the Midgut if SMA is Ligated Proximally
- Stable: Primary Repair vs Bypass Graft (Saphenous Vein or PTFE)
- Zone III/IV (Distal to the Middle Colic): Primary Repair vs Ligation
- Stable: Primary Repair
- Damage Control: Ligation
- Ligation of the Distal SMA is Poorly Tolerated and May Require Extensive Bowel Resection as it is Distal to the Collaterals
Inferior Mesenteric Artery (IMA)
- Small (< 50% Diameter): Lateral Arteriorrhaphy (Primary Repair)
- Large (> 50% Diameter): Ligate
Iliac Artery (Common/CIA or External/EIA)
- Small (< 50% Diameter): Lateral Arteriorrhaphy (Primary Repair)
- Large (> 50% Diameter): Patch Angioplasty vs Interposition Graft (Saphenous Vein or PTFE)
- Additional Options:
- Replace with Mobilized Ipsilateral Internal Iliac Artery
- Transposition to the Contralateral Iliac Artery if Injury is at the Bifurcation
- May Consider Extra-Anatomic Bypass if Significant Contamination is Present
- Additional Options:
Internal Iliac Artery (IIA)
- Can Ligate Both Internal Iliac Arteries with Near Impunity
The Use of Endovascular Repair for Abdominal Vascular Injury is Evolving but May Be Considered for Select Injuries
Aorta
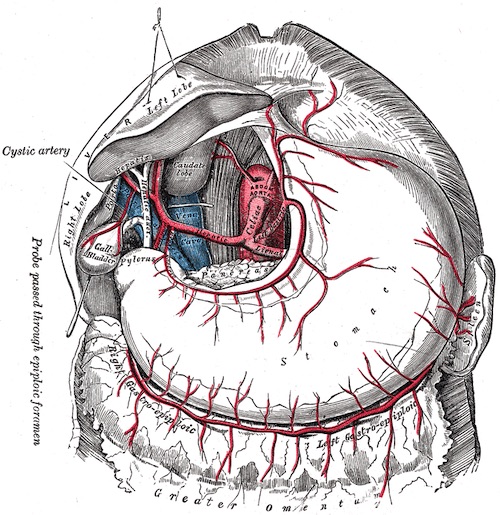
Celiac Axis
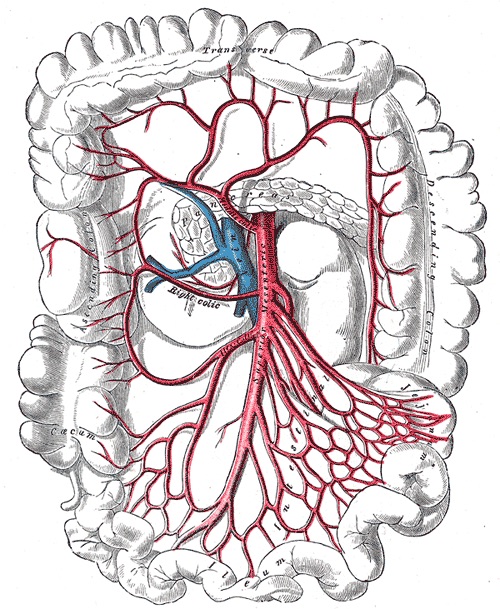
Superior Mesenteric Artery (SMA)

Inferior Mesenteric Artery (IMA)
Venous Injury
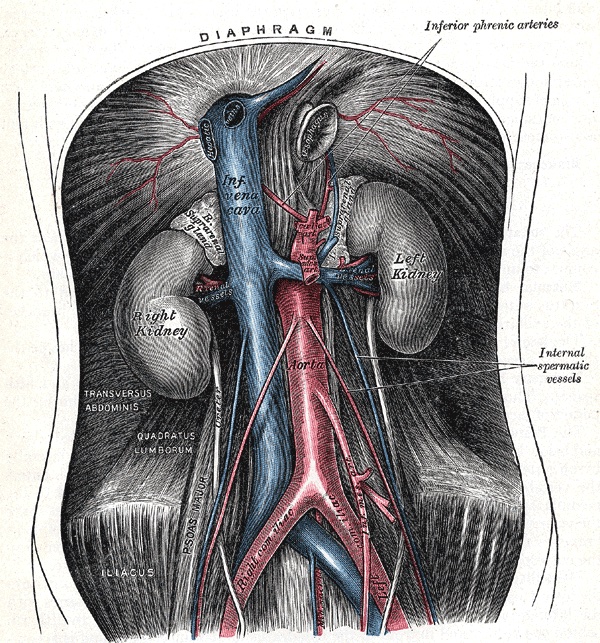
Retrohepatic Inferior Vena Cava (IVC)
Infrahepatic Inferior Vena Cava (IVC)
- Primary Treatment: Lateral Venorrhaphy (Primary Repair)
- Severe Injuries > 50% Diameter May Require Patch Venorrhaphy or Interposition Graft (Saphenous Vein or Synthetic Patch)
- Damage Control: Infrarenal Ligation
- Monitor for Compartment Syndrome and Consider Prophylactic Fasciotomy
- Considerations:
- Apply Pressure to Stop Bleeding – Do Not Clamp as it Will Tear Easily
- Posterior Wall Injury May Require Cutting Through the Anterior Wall to Access
- May Require Division of the Right Common Iliac Artery to Visualize the Distal IVC or Bifurcation
- Primarily Repair the Artery Later
Iliac Veins
- Primary Treatment: Lateral Venorrhaphy (Primary Repair)
- Severe Injuries > 50% Diameter May Require Patch Venorrhaphy or Interposition Graft (Saphenous Vein or Synthetic Patch)
- Damage Control: Ligation
- Monitor for Compartment Syndrome and Consider Prophylactic Fasciotomy
Renal Veins
- Primary Treatment: Lateral Venorrhaphy (Primary Repair)
- Damage Control: Ligation
- Left Renal Vein: Ligate Near the IVC and Spare the Kidney (Good Collaterals Through the Adrenal/Gonadal Veins)
- Right Renal Vein: Also Requires a Nephrectomy (Shorter than the Left with Poor Collaterals)
Can Ligate Any Vein Distal to the Renal Veins If Necessary for Damage Control (Including the IVC)
Portal System (Portal Vein, SMV, and IMV)
- Primary Treatment: Lateral Venorrhaphy (Primary Repair)
- Severe Injuries > 50% Diameter May Require Patch Venorrhaphy or Interposition Graft (Saphenous Vein or Synthetic Patch)
- Damage Control: Ligation – Will Cause Massive Bowel Edema and High Risk for Mesenteric Ischemia
- May Require Division of the Pancreas Neck to Access the Portal Vein
Inferior Vena Cava (IVC)
Portal System

