Ventilator Modes
Ventilator Modes
David Ray Velez, MD
Table of Contents
Overview
Volume Control (VC) vs. Pressure Control (PC)
- Controlled Mechanical Ventilation (CMV)
- Assist-Control Ventilation (AC)
- Synchronized Intermittent Mechanical Ventilation (SIMV)
Overview
There are 3 Primary Questions to Understand the Traditional Modes of Mechanical Ventilation
- Is the Ventilator Ensuring Delivery of Minimum Breaths (Controlled) or Just Supporting the Patient’s Own Breaths (Non-Controlled)?
- For Controlled Modes, Does the Ventilator Use Volume or Pressure to Deliver the Breaths
- For Controlled Modes, What Happens if the Patient Tries to Trigger a Spontaneous Breath
Definitions
- Minute Ventilation (MV): Amount of Air that Enters the Lungs per Minute
- MV = RR x Vt
- Respiratory Rate (f/RR): Number of Breaths Delivered per Minute
- Tidal Volume (Vt): Volume of Air Delivered with Each Breath
- Pressure Support (PS): Additional Pressure Added to PEEP to Cause Inspiration
- Also Known as Inspiratory Pressure (PI) or Change in Pressure (∆P)
- Positive End Expiratory Pressure (PEEP): Positive Pressure Remaining in Airways at the End of Expiration
- Fraction of Inspired Oxygen (FiO2): Percentage of Oxygen in Air Delivered to the Patient
- *See Ventilator Settings
Breath Types
- Patient-Trigger Breath: A Breath Initiated by the Patient’s Own Respiratory Drive (Can Be Triggered by Pressure Changes, Flow Changes, Volume Changes, or Shape-Signal)
- Machine-Triggered Breath: A Breath Automatically Cycled by the Ventilator without Any Patient Initiation
Controlled Modes
- Traditional Modes
- Controlled Mechanical Ventilation (CMV)
- Assist-Control Ventilation (AC)
- Synchronized Intermittent Mechanical Ventilation (SIMV)
- *Any of These Traditional Modes Can Be Either Volume-Controlled (VC) or Pressure-Controlled (PC)
- Advanced Modes
- Airway Pressure Release Ventilation (APRV)
- High-Frequency Oscillatory Ventilation (HFOV)
- Pressure-Regulated Volume-Controlled Ventilation (PRVC)
- Adaptive Support Ventilation (ASV)
- Minimum/Mandatory Minute Ventilation (MMV)
- Neurally Adjusted Ventilatory Assist (NAVA) Ventilation
Non-Controlled Modes
- Continuous Positive Airway Pressure (CPAP)
- Pressure Support Ventilation (PSV)
- CPAP with PSV (Similar to BPAP)
- Volume Support Ventilation (VSV)
- Proportional Assist Ventilation (PAV)
- Automatic Tube Compensation (ATC)
Open- vs. Closed-Loop Concept
- Open-Loop Modes: “Set and Deliver” – The Ventilator Does Not Adapt to the Patient Response
- Includes the Majority of Standard Modes
- Simpler but Requires More Frequent Adjustments
- Ex: CMV, AC, SIMV, PRVC, APRV, HFOV, CPAP, PSV
- Closed-Loop Modes: The Ventilator Uses Feedback from the Patient to Adapt the Support Provided
- A More Modern Concept for Newer Modes
- More Complex to Understand but Adapts Automatically to Reduce the Need for Constant Manual Adjustments
- May Shorten Weaning Times and Improve Synchrony
- Ex: ASV, MMV, NAVA, VSV, PAV
Volume Control (VC) vs. Pressure Control (PC)
Volume-Controlled (VC) Ventilation: Provides a Set Tidal Volume for the Given Inspiratory Time
- Advantages:
- Tidal Volume is Set with a Guaranteed Minute Ventilation
- Easier to Predict CO2 Elimination and Manage Acid-Base Balances
- Disadvantages:
- Variable (Possibly High) Peak Inspiratory Pressure (PIP) with Increased Risk for Barotrauma
- Decreased Comfort and Possibly Increased Work of Breathing
- May See Patient-Ventilator Dyssychrony
Pressure-Controlled (PC) Ventilation: Provides a Set Inspiratory Pressure for the Given Inspiratory Time
- Advantages:
- Peak Inspiratory Pressure (PIP) is Constant (PIP = Inspiratory Pressure + PEEP)
- Decreased Risk for Barotrauma by Lower PIP
- Increased Mean Airway Pressure and Duration of Alveolar Recruitment
- Increased Comfort and Decreased Work of Breathing
- May Allows Better Synchrony with the Ventilator
- Disadvantages:
- Tidal Volume is Variable Depending on Lung Compliance and Resistance
- Minute Ventilation is Therefore Unpredictable, and it May Be More Difficult to Predict CO2 Elimination
- Risk for Hypoventilation or Hyperventilation
- Needs Close Monitoring and May Require More Frequent Adjustments
The Traditional Modes (CMV, AC, and SIMV) Can Be Set Using Either Volume-Control (VC) or Pressure-Control (PC) to Deliver Breaths
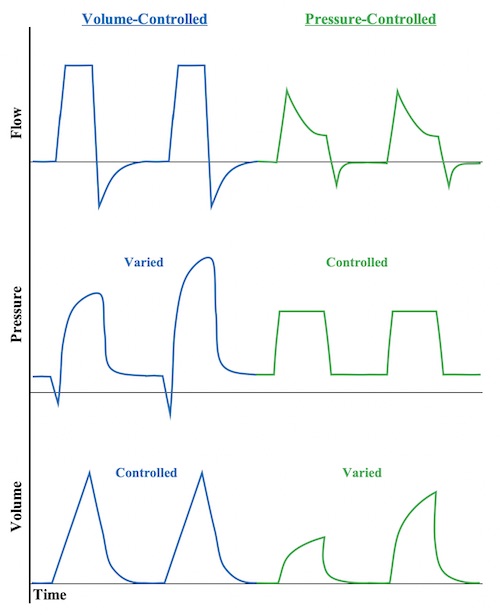
Time Graphs of Volume- vs Pressure-Controlled Ventilation 5
Controlled Mechanical Ventilation (CMV)
The First Modern Mechanical Ventilator Mode From the 1940’s but Generally Not Used in Modern Practice
Mechanism
- Delivers a Controlled Number of Breaths at a Set Volume or Pressure
- Does Not Allow Any Patient-Triggered Breaths
Advantages
- Lowest Work of Breathing
- Set Minute Ventilation is Easily Adjusted
Disadvantages
- Uncomfortable and May Cause Significant Ventilator Dyssynchrony with Wasted Effort
- May Require Deeper Sedation or Paralytics
Original Use: Controlled Mechanical Ventilation (CMV) is the Original Mode Used in the 1980-1990’s That Provided No Assist and is Not Used in Modern Practice Modern Practice: Continuous Mandatory Ventilation (CMV/CMV+) Has Now Been Adopted by Many Modern Manufacturers as Another Name for Assist Control (AC) |
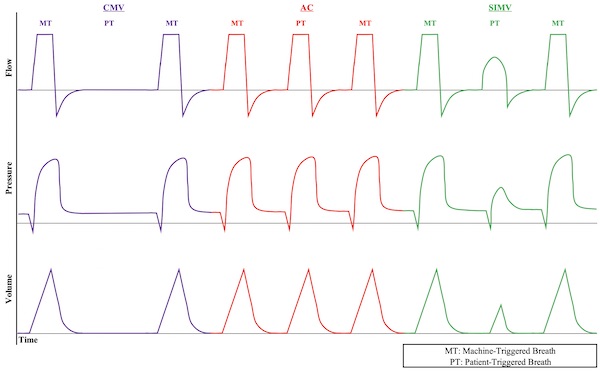
Time Graphs of Volume-Controlled Ventilation Modes 5
Assist-Control Ventilation (AC)
Also Known as: Continuous Mandatory Ventilation (CMV/CMV+)
Mechanism
- Delivers a Minimum Number of Breaths at a Set Volume or Pressure
- Allows Patient-Triggered Breaths in Addition to Set Minimum Breaths
- Patient-Triggered Breaths are at the Set Volume
Advantages
- Increased Comfort and Useful for Awake Patients with Spontaneous Breathing
- Allows Sedation Weaning
- Improved Ventilator Synchrony
- Lower Work of Breathing than SIMV
Disadvantages
- Higher Work of Breathing than CMV
- Can Hyperventilate with Respiratory Alkalosis if Patient Overbreathes
- Risk for Auto-PEEP or Dynamic Hyperinflation in Obstructive Lung Disease
Time Graphs of Volume-Controlled Ventilation Modes 5
Synchronized Intermittent Mechanical Ventilation (SIMV)
- Delivers a Minimum Number of Breaths at a Set Volume or Pressure
- Allows Patient-Triggered Breaths in Addition to Set Minimum Breaths
- Patient-Triggered Breaths are at the Patient’s Own Volume with or without Pressure Support
- May Allow “Exercise of Respiratory Muscles” Although There is No Proven Advantage to SIMV 4
- Highest Work of Breathing of Traditional Modes and Can Cause Respiratory Fatigue
- Less Comfortable than AC
- Can Hyperventilate with Respiratory Alkalosis if Patient Overbreathes
| Intermittent Mechanical Ventilation (IMV): Mandatory Breaths are at Fixed Times with No Synchronization to Patient Effort – Uncomfortable and Not Used in Modern Practice |
Time Graphs of Volume-Controlled Ventilation Modes 5
Airway Pressure Release Ventilation (APRV)
Mechanism
- Maintains High Pressure (P High) for an Extended Time (T High) to Optimize Oxygenation
- Pressure Released (P Low) for a Short Period of Time (T Low) to Allow Ventilation
- Longer Inspiratory/Expiratory Ratio: 80-95%
- Spontaneous Breathing is Permitted but Will Have Low Tidal Volumes at the Higher Pressures
Most Commonly Used for Severe ARDS When Having Difficulty Oxygenating on Other Modes 6,7
General Settings
- P High: 25-35 cmH2O
- T High: 4.5-6.0 Seconds
- P Low: 0-5 cmH2O
- T Low: 0.5-0.8 Seconds
- FiO2: Adjusted as Needed, Start at 100% and Titrate Down Based Upon ABG and Pulse Oximetry as Able
- Keep Automatic Tube Compensation (ATC) on if Spontaneously Breathing
General Management
- Increase Oxygenation:
- Increase FiO2 (Max 100%)
- Increase P High (Max 30-35 cmH2O)
- Increase T High (Max 6 Seconds)
- Increase Ventilation (Decrease CO2):
- Increase the Gradient Between P High and P Low
- Decrease T High
- Increase T Low
- *In General, APRV is Avoided if Needing High Ventilatory Requirements
Advantages
- Maximize Alveolar Recruitment and Oxygenation
- Lung-Protective with Lower Peak Pressures and Less Barotrauma
- More Comfortable than Traditional Modes (CMV/AC/SIMV) Allowing for Greater Spontaneous Breathing and a More Natural Respiratory Pattern – Allows Decreased Sedation
Disadvantages
- Not Ideal if Requiring Heavy Sedation – Spontaneous Breathing is Important for Ventilation
- Generally Avoided in Severe Obstructive Airway Disease – Risks for Air Trapping with Hyperinflation, Increased Pressure, and Barotrauma
- Generally Avoided if Needing High Ventilatory Requirements – Risk for Hypercapnia Due to Shorter Expiratory Times
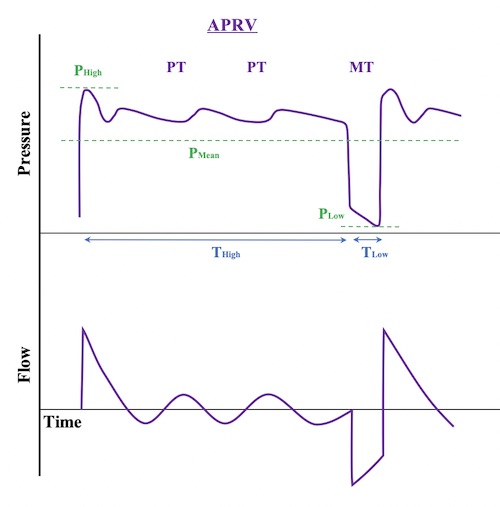
APRV Time Graphs 5
High-Frequency Oscillatory Ventilation (HFOV)
Mechanism
- Very High Respiratory Rate (300-900 Breaths per Minute) by a High-Frequency Oscillatory Pump
- Rate is So Fast That the Airway Pressure Merely Oscillates Around a Constant Mean Airway Pressure
- Does Not Produce Large Bulk Tidal Volumes but Rather Creates a Relatively Continuous Gas Flow
Most Commonly Used for Severe ARDS Only When Having Difficulty Oxygenating on Other Modes – Should Not Be Used Routinely and May Actually Increase Mortality 8,9
Less Commonly Used in Modern Practice
Settings
- Bias Flow: 30-40 L/min
- Frequency (F): 3-15 Hz (1 Hz is Equivalent to 60 Breaths per Minute)
- Inspiratory Time: 33% (I:E Ratio of 1:2)
- Mean Airway Pressure (MAP): 25-35 cmH2O
- Generally Started at 2-3 cmH2O Above the Prior MAP on CMV
- Power/Amplitude (Delta P): 30-90 cmH2O
- Sets the Variation Around the MAP
- Appropriate Amplitude is Based on “Chest Wiggle”/Vibration
- FiO2: Adjusted as Needed
General Management
- Increase Oxygenation:
- Increase FiO2 (Max 100%)
- Increase Mean Airway Pressure/MAP (Max 30-35 cmH2O)
- Increase Ventilation (Decrease CO2):
- Increase Power/Amplitude (Delta P) – Primarily
- Decrease Frequency – Increases Vt of Each Breath
- Increase Inspiratory Time (I:E Ratio) – Increases Vt of Each Breath (Risk for Air Trapping)
Advantages
- Maintains Alveolar Recruitment and Oxygenation
- Lung-Protective with Lower Peak Pressures and Less Barotrauma
Disadvantages
- Significant Discomfort and Requires Heavy Sedation or Paralysis
- Decreased Expiratory Time Creates Risk for Hyperinflation with Increased Pressure and Barotrauma
- High Risk of Hemodynamic Instability Due to High Mean Airway Pressures
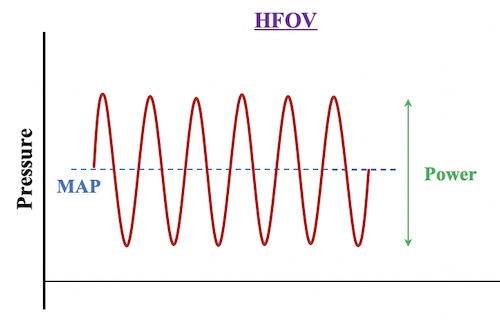
HFOV Pressure-Time Graph 5
Pressure-Regulated Volume-Controlled Ventilation (PRVC)
Also Known as: Volume Control Plus (VC+) or Adaptive Pressure Ventilation (APV)
A Method of Mechanical Ventilation that Combines Attributes of Both Volume-Control and Pressure-Control
Mechanism
- A Controlled Volume is Set (Similar to Volume Control)
- The Ventilator Attempts to Achieve the Target Volume Using a Pressure-Control Gas Delivery Format
- The Ventilator Continuously Adjusts the Pressure as Needed to Ensure the Lowest Possible Airway Pressure to Deliver the Set Volume
Benefits
- The Set Volume Ensures a Constant Tidal Volume and Minute Ventilation
- Using Pressure to Control Allows Variable Flow Rates and Reduced Work of Breathing
- Uses the Lowest Possible Pressure to Deliver the Set Volume to Decrease the Risk of Barotrauma
Other Controlled Modes
Adaptive Support Ventilation (ASV)
- Mechanism:
- Continual Adjustments are Automatically Made to Respiratory Rate and Inspiratory Pressure to Achieve a Goal Minimum Minute Ventilation (MMV)
- The Ventilator Calculates Optimal Settings by the “Otis Equation” to Minimize Work of Breathing
- Accounts for Respiratory Mechanics (Resistance, Compliance, Dead Space – Calculated)
- Patient-Triggered Breaths are Given Pressure Support as Needed
- Machine-Controlled Breaths are Given as Needed to Achieve a Calculated Respiratory Rate
- Described as a “No Mode” or “Meta-Mode” Because it is an Adaptive “Closed-Loop” Strategy that Continuously Transitions Between Modes Depending on Needs
- Settings:
- Ventilate by Setting a Percentage of Minimum Volume (MinVol) of Desired Minute Ventilation
- 100% Normal, 120% in ARDS, 90% in Asthma, 110% in Others
- Add 20% for Fevers > 101.3 F
- Oxygenate by Setting PEEP and FiO2
- Ventilate by Setting a Percentage of Minimum Volume (MinVol) of Desired Minute Ventilation
- Advantages:
- Decreased Work of Breathing
- Attempts Lung Protective Strategies to Prevent Volutrauma, Barotrauma and Auto PEEP
- May Decrease Ventilator Weaning Time in COPD
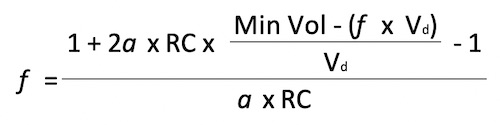
Otis Equation for Adaptive Support Ventilation 5
Minimum/Mandatory Minute Ventilation (MMV)
- A Minimum Minute Ventilation (MV) is Set (ex: 6 L/min)
- The Ventilator Monitors a Patient’s Spontaneous Breathing Volumes and Delivers Extra Mandatory Breaths if Spontaneous Ventilation is Below the Target
- Can Set Machine-Triggered Breaths to Be Either Volume-Controlled or Pressure-Controlled
- Primarily Used as a Weaning Mode and Not for Full Ventilator Support
- Comparison to SIMV:
- SIMV: A Fixed Number of Mandatory Breaths with Optional Spontaneous Breaths
- MMV: A Variable Number of Machine-Triggered Breaths in Addition to Spontaneous Breaths to Meet the Target Ventilation Goal
Neurally Adjusted Ventilatory Assist (NAVA) Ventilation
- Mechanism:
- Catheter Implanted in a Gastric Tube Detects Electrical Discharge in the Diaphragm
- Diaphragm Excitation Triggers a Mechanical Breath
- The Degree of Assist Varies by the Amplitude of the Electrical Discharge – Tidal Volumes Variable
- Advantages:
- Neural-Ventilator Coupling (Time Between Spontaneous Breath and Delivered Mechanical Breath) is Faster than Conventional Modes
- May Increase Ventilator Synchrony
- Disadvantages:
- Requires Spontaneous Breathing – Unable to Use with Heavy Sedation or Blunted Respiratory Drive
Non-Controlled Modes (CPAP/PSV)
Non-Controlled Modes of Ventilation are Primarily Used for Ventilator Weaning to Overcome the Resistance of the Endotracheal Tube and are Not Appropriate for Patients Requiring Significant Ventilatory Support
Disadvantages
- Higher Work of Breathing and Can Cause Respiratory Fatigue
- Can Result in Carbon Dioxide Retention and Acidosis
- Poor Choice for Full Ventilatory Support
Continuous Positive Airway Pressure (CPAP)
- Provides a Continuous Pressure Level (Similar to PEEP)
- All Breaths are Patient-Triggered – Patient Determines the Rate and Volume
- No Additional Support Provided to Patient-Triggered Breaths
- General Settings:
- CPAP: 5-15 cmH2O
- FiO2: Adjusted as Needed
Pressure Support Ventilation (PSV)
- Additional Pressure Support Provided to Patient-Triggered Breaths
- All Breaths are Patient-Triggered – Patient Determines Rate and Volume
- General Settings:
- Pressure Support: 5-20 cmH2O
- FiO2: Adjusted as Needed
- CPAP with PSV (Similar to BPAP)
- Pressure Support is Added in Addition to PEEP
- PSV 10/5 Indicates 5 cmH2O of PEEP and 15 cmH2O During Support
Volume Support Ventilation (VSV)/Volume Targeted Ventilation (VTV)
- Continuously Adjusts Pressure Support to the Level Needed to Achieve a Target Tidal Volume
- Some Evidence Suggests Decreased Weaning Time and Total Ventilation Time
- Significant Literature Evaluating its Use in Neonates
Proportional Assist Ventilation (PAV)
- The Ventilator Delivers Additional Pressure Proportional to a Patient’s Effort
- Set the “Gain”: Percentage of Assistance to Patient Effort
- No Fixed Pressure or Volume Target (vs PSV/VSV)
- Often Described as “Power Steering” for Breathing
Automatic Tube Compensation (ATC)
- Ventilator Programming Continuously Adjusts Pressure Support to the Level Needed to Overcome the Endotracheal Tube
- ATC Can Be Used as a Component and Combined with Any Conventional Ventilator Mode
References
- Sancar NK, Özcan PE, Şentürk E, Selek Ç, Çakar N. The Comparison of Pressure (PSV) and Volume Support Ventilation (VSV) as a ‘Weaning’ Mode. Turk J Anaesthesiol Reanim. 2014 Aug;42(4):170-5.
- Peng W, Zhu H, Shi H, Liu E. Volume-targeted ventilation is more suitable than pressure-limited ventilation for preterm infants: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2014 Mar;99(2):F158-65.
- Klingenberg C, Wheeler KI, McCallion N, Morley CJ, Davis PG. Volume-targeted versus pressure-limited ventilation in neonates. Cochrane Database Syst Rev. 2017 Oct 17;10(10):CD003666.
- de Godoi TB, Marson FAL, Palamim CVC, Cannonieri-Nonose GC. Influence of ventilatory strategies on outcomes and length of hospital stay: assist-control and synchronized intermittent mandatory ventilation modes. Intern Emerg Med. 2021 Mar;16(2):409-418.
- Velez DR. Mechanical Ventilation: Modes. The Operative Review of Surgery. 2023.
- Mireles-Cabodevila E, Dugar S, Chatburn RL. APRV for ARDS: the complexities of a mode and how it affects even the best trials. J Thorac Dis. 2018 Apr;10(Suppl 9):S1058-S1063.
- Zhou Y, Jin X, Lv Y, Wang P, Yang Y, Liang G, Wang B, Kang Y. Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome. Intensive Care Med. 2017 Nov;43(11):1648-1659.
- Sklar MC, Fan E, Goligher EC. High-Frequency Oscillatory Ventilation in Adults With ARDS: Past, Present, and Future. Chest. 2017 Dec;152(6):1306-1317.
- Ng J, Ferguson ND. High-frequency oscillatory ventilation: still a role? Curr Opin Crit Care. 2017 Apr;23(2):175-179.
- Otis AB, Fenn WO, Rahn H. Mechanics of breathing in man. J Appl Physiol. 1950;2:592–607.
- Tehrani FT, Roum JH. Flex: A new computerized system for mechanical ventilation. J Clin Monit Comput. 2008;22:121–30.

