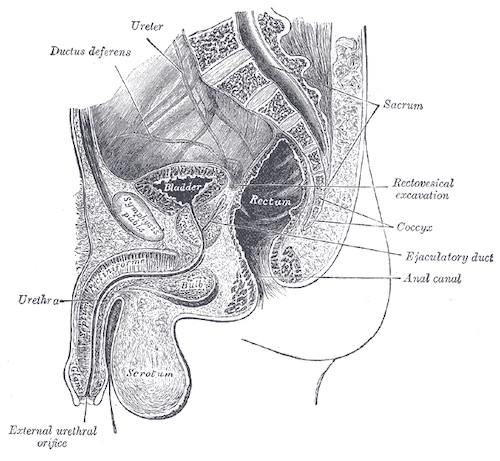
Urethra Anatomy

Butterfly Perineal Hematoma 1

Urethral Injury on Retrograde Urethrogram: Partial (Left) and Complete (Right) 2
Urethra Anatomy
Butterfly Perineal Hematoma 1
Urethral Injury on Retrograde Urethrogram: Partial (Left) and Complete (Right) 2

