Lower 1/3 (Below Pelvic Brim): Ureteroneocystostomy (Reimplant in Bladder)
*See Techniques Below
Damage Control Options
Cutaneous Ureterostomy – Stent Placed Through the Proximal Transected Ureter and Externalized to Control Urinary Output Until Stabilized for Delayed Definitive Repair
Ligate Ends with a Percutaneous Nephrostomy
Surgical Technique
Always Use Absorbable Sutures – Avoid Stricture/Stones
Avoid Skeletonization When Dissecting – Risk for Devascularization
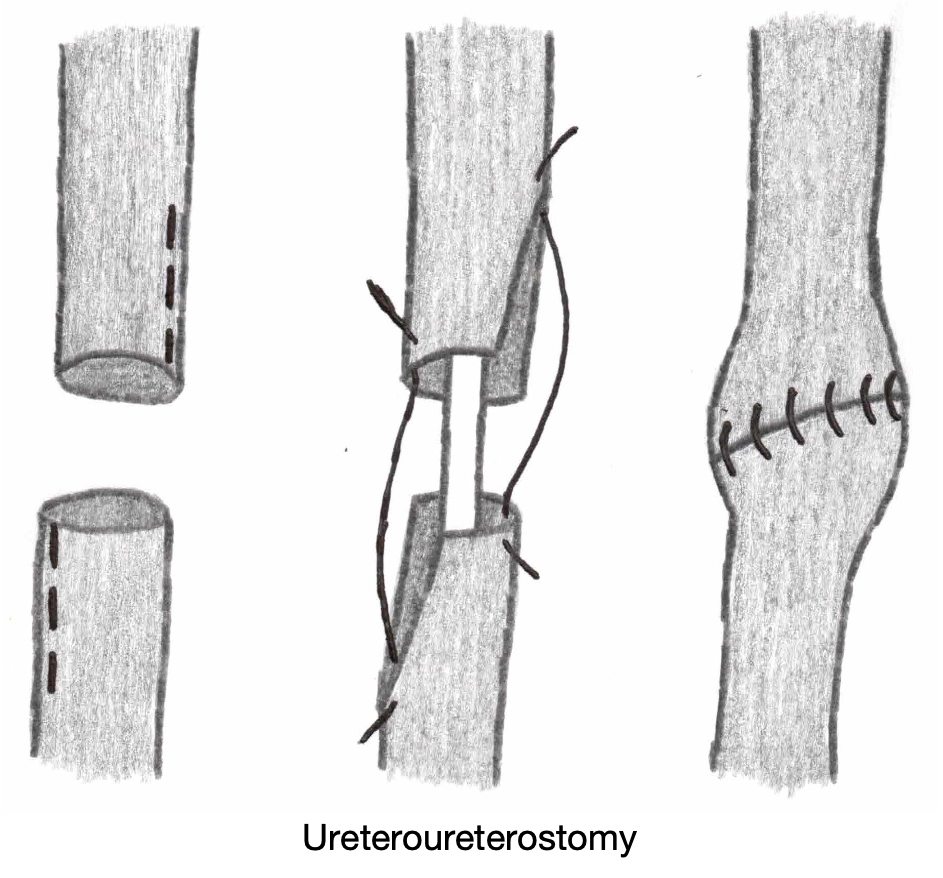
Ureteroureterostomy
Definition: Ureter-to-Ureter Anastomosis
Debride Devitalized Tissue
Spatulate the Proximal and Distal Ends
Insert a Double-J Ureteral Stent
Create the Anastomosis Over the Stent
Use Absorbable Monofilament Sutures (PDS 5-0) to Avoid Stricture/Stones
*Large Injuries May Require Kidney Mobilization and Nephropexy to Decrease Tension
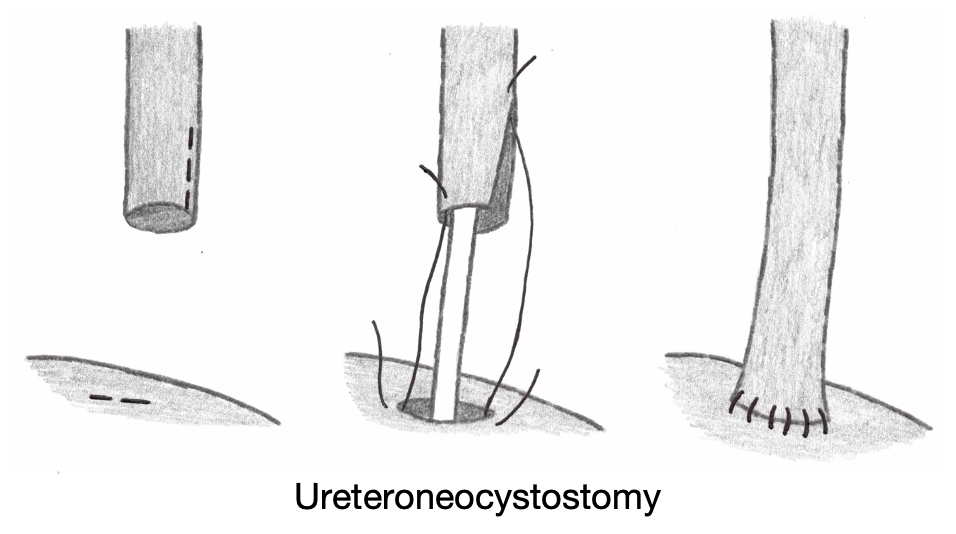
Ureteroneocystostomy
Definition: Ureter Reimplantation into the Bladder
Debride Devitalized Tissue
Spatulate the Proximal End of the Ureter
Create a Small Cystotomy
Insert a Double-J Ureteral Stent
Anastomose the Ureter to the Bladder Cystotomy Over the Stent
Use Absorbable Monofilament Sutures (PDS 5-0) to Avoid Stricture/Stones
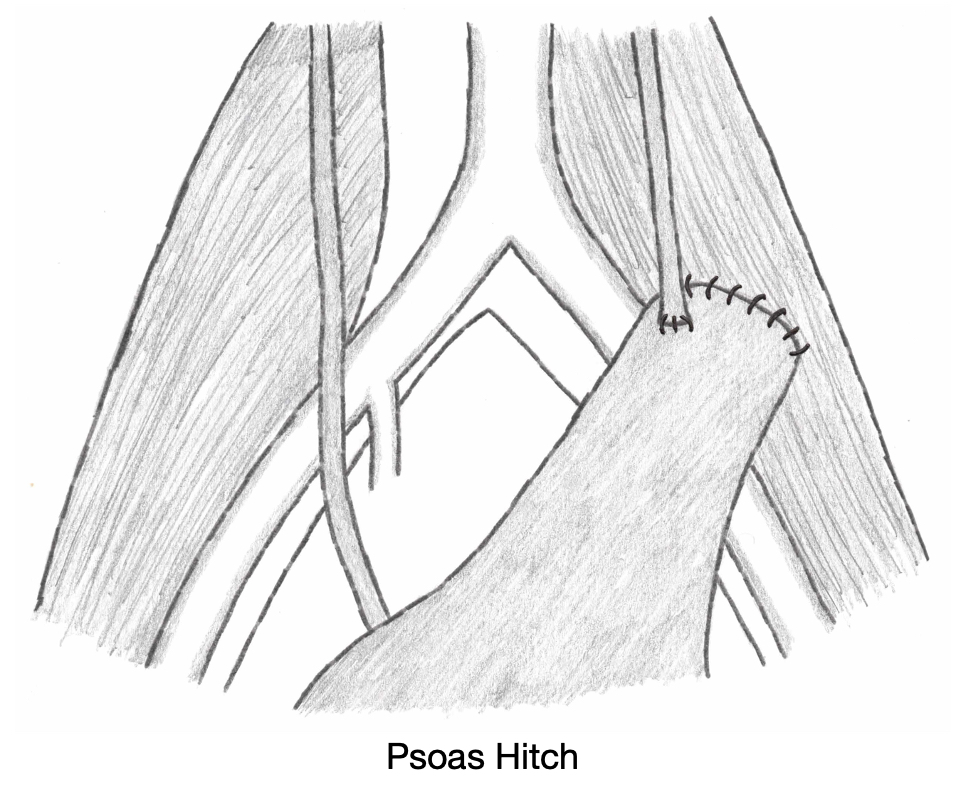
Adjuncts to Decrease Tension for Large Defects
Psoas Hitch– Mobilize Bladder and Anchor to the Psoas (Generally Preferred)
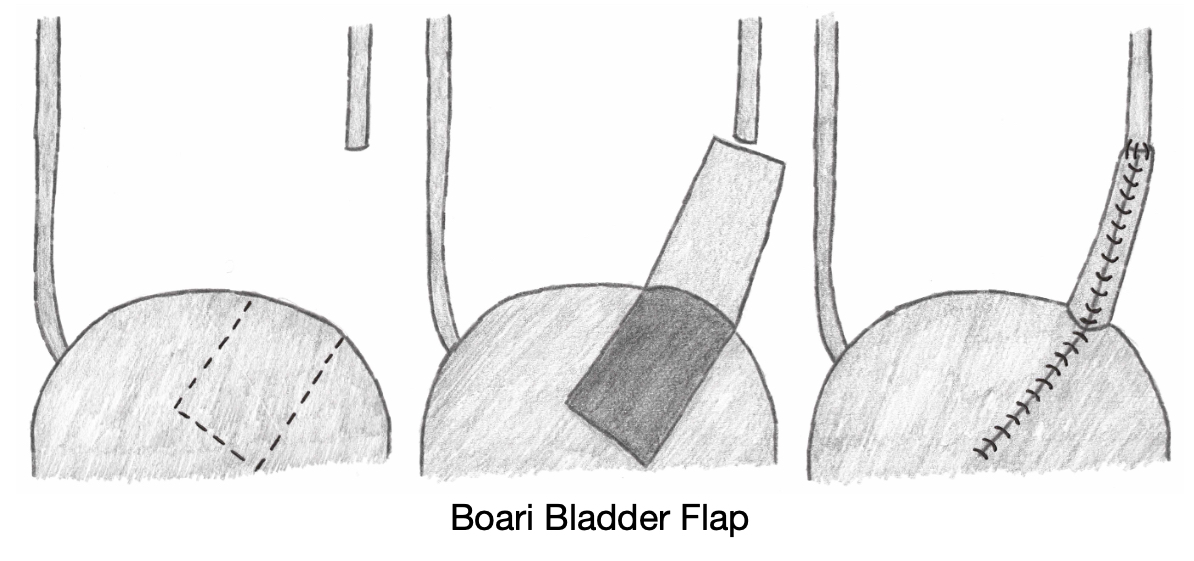
Bladder (Boari) Flap – Bladder is Tubularized
Transureteroureterostomy (TUU) – Implant into the Contralateral Ureter
Ileal Interposition
Renal Autotransplantation – Autotransplant of the Ipsilateral Kidney into the Pelvis
References
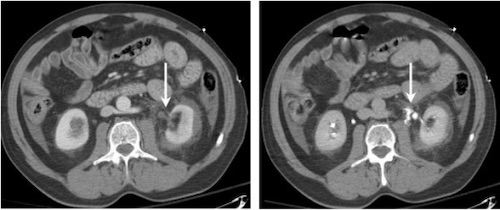
Ortega SJ, Netto FS, Hamilton P, Chu P, Tien HC. CT scanning for diagnosing blunt ureteral and ureteropelvic junction injuries. BMC Urol. 2008 Feb 7;8:3. (License: CC BY-2.0)