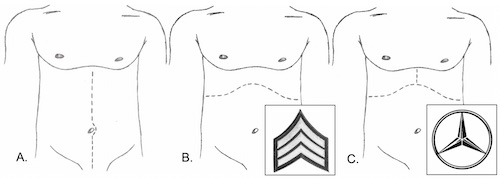
Incisions: (A) Midline, (B) Chevron, (C) Mercedes
Supraceliac Control of the Aorta
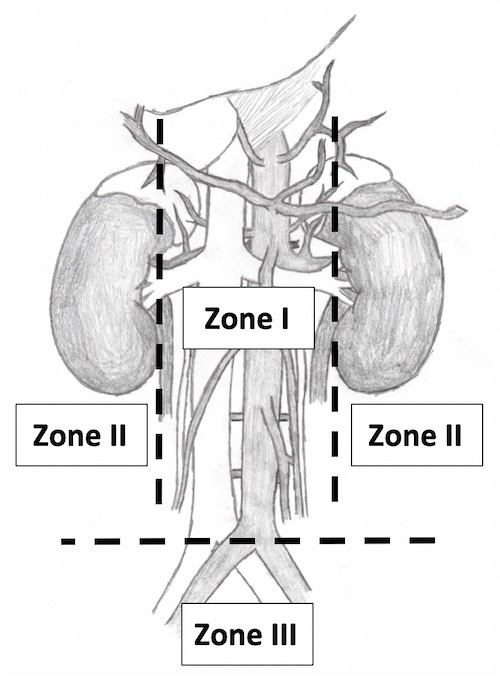
Retroperitoneal Zones

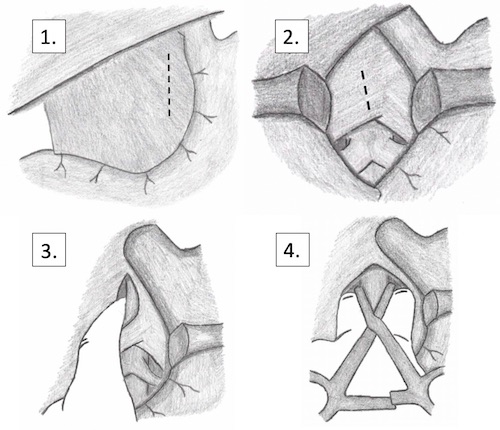
Maneuvers to Access the Retroperitoneum: 1. Mattox, 2. Cephalad Transverse Mesocolon Reflection, 3. Kocher*, 4. “Extended” Kocher*, 5. “Super-Extended” Kocher*, *#3-5 Together Compose the Cattell-Braasch Maneuver