Laryngotomia by Julius Casserius (1552-1616)

Tracheostomy Material: Shiley (Left), Bivona (Middle), Jackson (Right)

Tracheostomy Cuff: Cuffed (Left), Uncuffed (Right)

Tracheostomy Fenestration: Fenestrated (Left), Non-Fenestrated (Right)
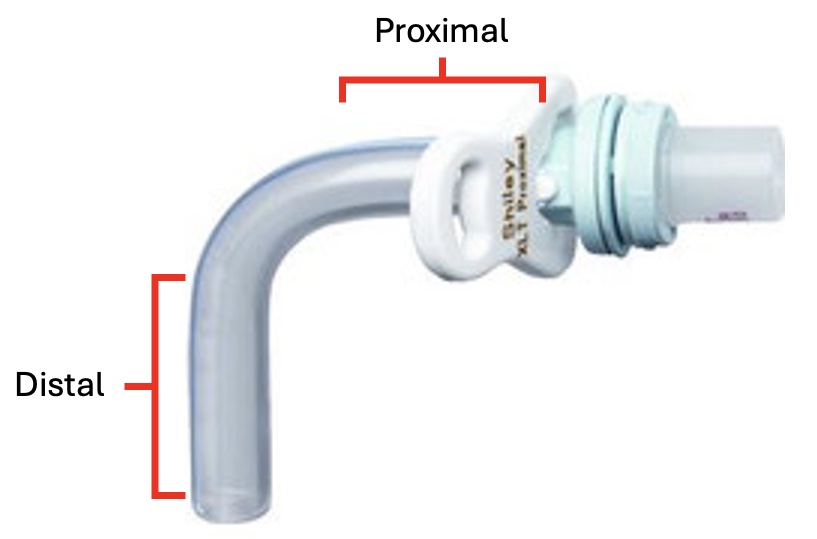
Tracheostomy Length
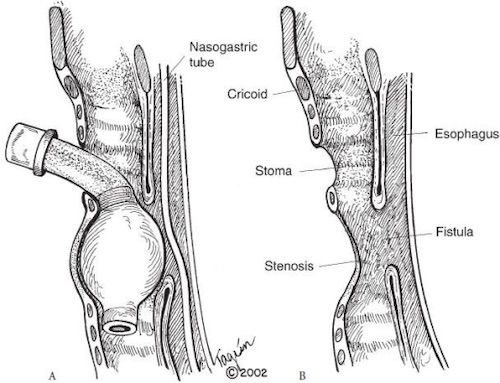
Tracheoesophageal Fistula (TEF) 1