Thoracic Vascular Injury
Thoracic Vascular Injury
David Ray Velez, MD
Table of Contents
Background
Thoracic Vascular Injury Has High Mortality and Cause 50% of All Trauma Deaths
Nearly All Thoracic Vascular Injuries Have Other Associated Injuries and Rarely Occur in Isolation
Etiology
- Over 90% are Due to Penetrating Trauma or Iatrogenic Injury
- Most Common Thoracic Great Vessel Injury by Mechanism:
- Stab Wounds: Ascending Aorta
- Gunshot Wounds: Descending Aorta
- Blunt Thoracic Trauma: Aortic Isthmus (Just Beyond Left Subclavian Takeoff)
AAST Thoracic Vascular Injury Scale
- *See AAST
- Injury Scale is Under Copyright
Initial Evaluation and Management
Indications for Immediate Resuscitative Thoracotomy: *See Resuscitative Thoracotomy
Screening Techniques
- History and Physical Exam
- Chest X-Ray (CXR)
- Focused Assessment with Sonography in Trauma (FAST)
CXR Findings Suggestive of Vascular Injury
- Indistinct Aortic Knob
- Wide Mediastinum > 8 cm
- Left Main Bronchus Depression > 140 Degrees
- Deviation of NG/ET Tubes to the Right
- Massive Hemothorax
If History and Physical Exam is Suggestive of Blunt Thoracic Aortic Injury Start Anti-Impulse Therapy if Otherwise Stable, Even Before Definitive Diagnosis
Massive Hemothorax – Thoracotomy Indications
- Initial Loss > 1,500 cc
- Continual Loss > 200 cc/hr for 4 Hours
- *Some Say 250 cc/hr for 3 Hours
- CAUTION: A Dramatic Decrease in Volume Can Be Due to Complete Evacuation but Can Also Occur Due to Clotting within the Chest Tube
- *See Hemothorax (HTX)
May Be Diagnosed on CT/CTA or Intraoperatively if Unstable or in Extremis
May Consider Catheter Angiography or Transesophageal Echocardiogram (TEE) if Initial Imaging is Equivocal
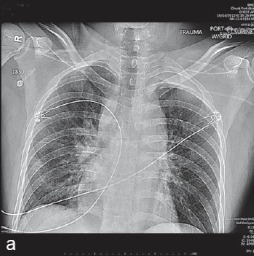
Thoracic Vascular Injury on CXR (Indistinct Aortic Knob and Widened Mediastinum 1
Definitive Management
Endovascular Techniques are Evolving and May Be Considered for Stable Patients with Select Injuries – Most Often Used for Small Partial Injuries but Have Also Been Used for Complete Transection or Thrombosis by Advanced Through-and-Through Snare Techniques
Blunt Thoracic Aortic Injury (BTAI)
Operative Sequence
- Step 1. Temporary Bleeding Control
- Manual Pressure
- Wound Packing
- Hemostatic Dressings (QuickClot Combat Gauze)
- Foley Balloon Catheter Inserted into the Wound if Deep and Narrow
- Step 2. Extensive Exposure
- Step 3. Definitive Control (Proximal and Distal)
- Step 4. Decision (Definitive Repair vs Damage Control)
Vascular Exposure
Surgical Management: Artery Injury
- Small Injuries (< 50% Circumference): Arteriorrhaphy (Primary Repair)
- Large Injuries (> 50% Circumference or Transection): Interposition or Dacron Bypass Grafting
- May Consider Subclavian Artery or Internal Mammary Artery (IMA) Ligation in Damage Control
Surgical Management: Venous Injury
- Simple Venous Injuries Can Be Repaired by Lateral Venorrhaphy
- The Majority of Veins (Besides the SVC and Innominate) Can Be Managed by Simple Ligation if Complex or Hemodynamically Unstable
- Decision is Made for Surgical Repair vs Ligation Based on Severity of Injury and Hemodynamic Status
- Complex Injuries to the SVC or Innominate May Require PTFE Patch or a Dacron Interposition Graft
References
- Alameddine AK, Alimov VK, Alvarez C, Rousou JA. Unexpected traumatic rupture of left atrium mimicking aortic rupture. J Emerg Trauma Shock. 2014 Oct;7(4):310-2. (License: CC BY-NC-SA-3.0)