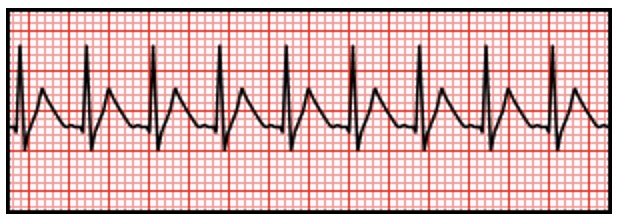
Supraventricular Tachycardia (SVT) Supraventricular Tachycardia (SVT) David Ray Velez, MD A Rapid Rhythm that Originates from Foci at or Above the Atrioventricular (AV) NodeThe Term “SVT” is Often Mistakenly Used Synonymously with Atrioventricular Nodal Reentrant Tachycardia (AVNRT) – A Type of SVTSinus Tachycardia and Atrial Fibrillation are Technically Types of SVTTypesAtrial Origin, Regular Rhythm:Sinus TachycardiaAtrial FlutterFocal Atrial TachycardiaSinoatrial Nodal Reentry Tachycardia (SNART)Atrial Origin, Irregular Rhythm:Atrial FibrillationMultifocal Atrial Tachycardia (MAT)AV Nodal Origin, Regular Rhythm:Atrioventricular Nodal Reentrant Tachycardia (AVNRT)Atrioventricular Reentrant Tachycardia (AVRT)Junctional Ectopic TachycardiaGeneral EKG PatternHeart Rate > 100 bpmNarrow QRS Complex (< 120 ms)Compared to Sinus Tachycardia:Often Has No Identified Underlying CauseSudden OnsetRate is Usually Very High > 150 bpmTypically See Combined P and T WavesGenerally Symptomatic (Chest Pain, Dyspnea, Anxiety)Often Has Limited Rate Variability Supraventricular Tachycardia (SVT) TreatmentUnstable: Synchronized CardioversionStable: Vagal Maneuvers and AdenosineTry Vagal Maneuvers Initially and then Give Adenosine if FailsEx: Carotid Massage or Valsalva Maneuver12-18% SuccessAdenosine Dosing: 6 mg IV Rapidly Over 1-3 SecondsCan Repeat with 12 mg Doses if NeededDecrease Dose by 50% if Given Through a Central Line (3 mg/6 mg)*See Antiarrhythmic Pharmacology