
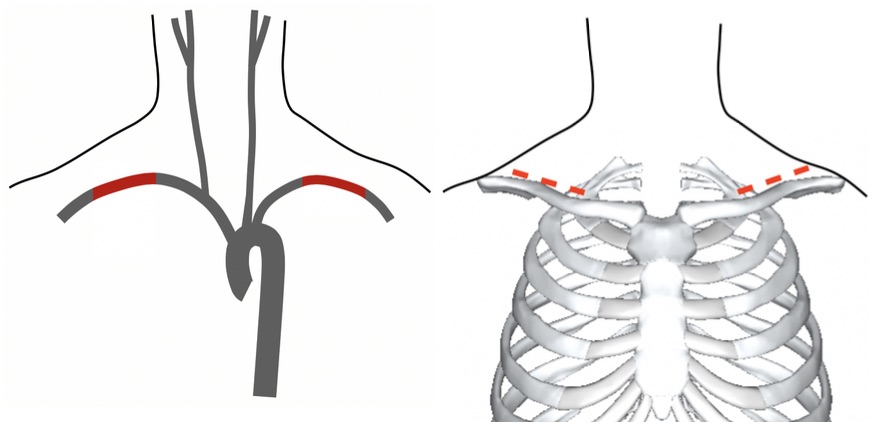
Exposure by Median Sternotomy
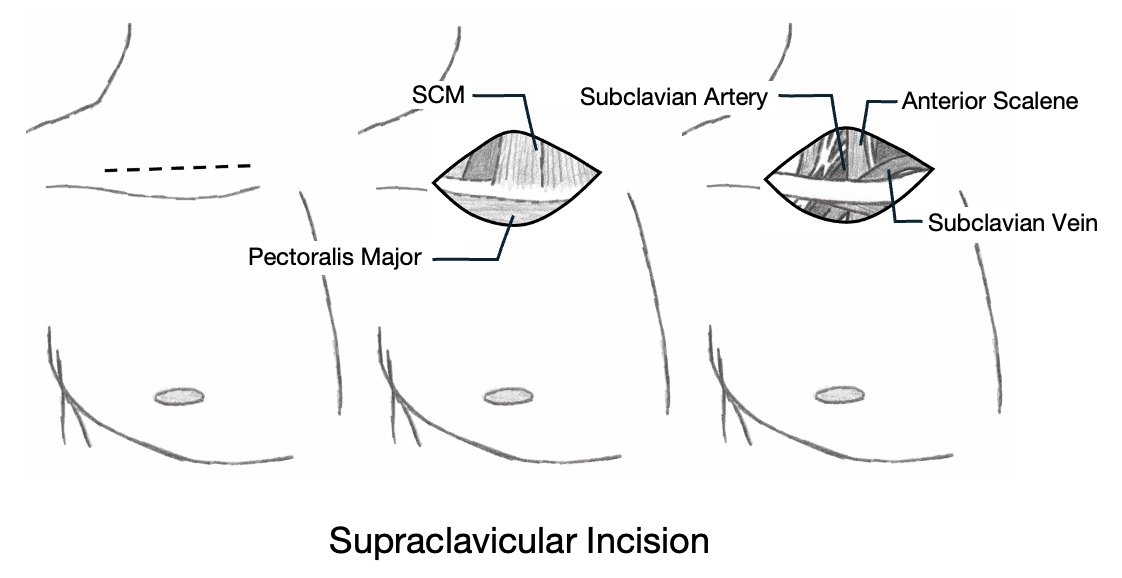
Exposure by Supraclavicular Incision
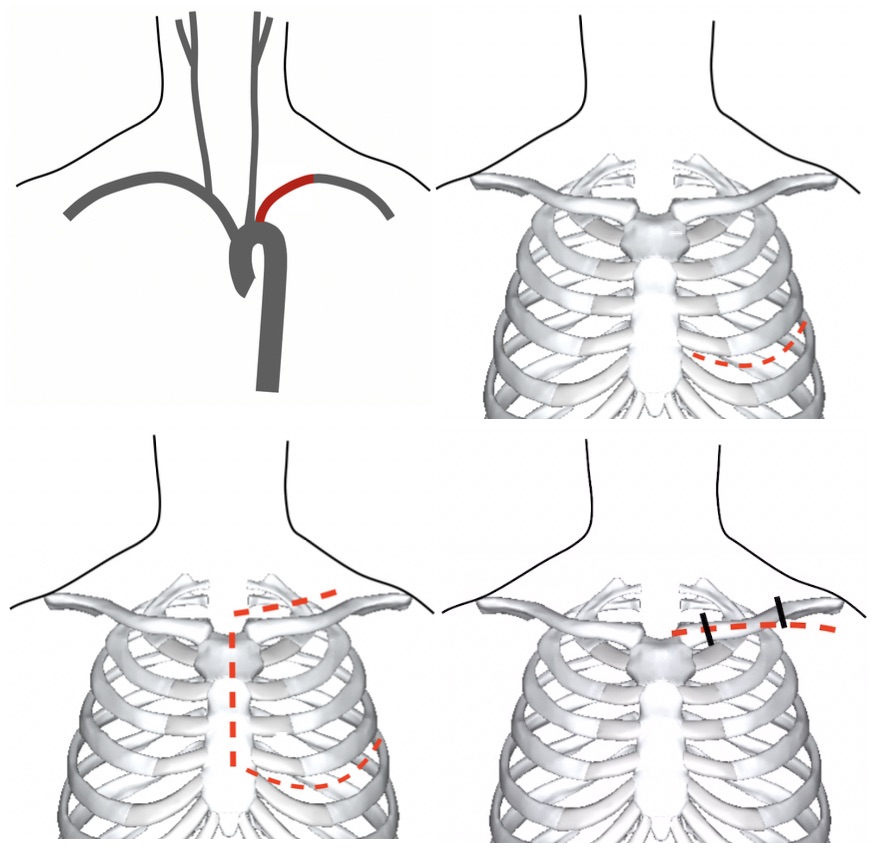
Access to the Left Subclavian (Thoracotomy, Trap Door, and Clavicular Incision)
Exposure by Median Sternotomy
Exposure by Supraclavicular Incision
Access to the Left Subclavian (Thoracotomy, Trap Door, and Clavicular Incision)