Unless the Stomach is Full, there is a High Blunt Force, or Seat Belts are Worn Improperly
In Blunt Stomach Injuries, there are Often Concomitant Injuries to Other Organs in the Abdomen or Chest Due to the High Blunt Force Required
Mechanism of Injury
Penetrating Mechanisms:
Direct Injury – Tearing & Crushing Force Through Tissue Along the Trajectory of the Projectile & its Fragments
Gunshot Wounds Have an Additional Dissipation of Kinetic Energy That Causes Further Damage
Cavitation – As a High Energy Projectile Moves Through Tissue Energy Causes a Radial Stretching, Forming a Temporary Cavity with Additional Tissue Damage
Higher Energy Projectiles Create Larger Cavities & Cause More Damage
Shock Wave – The Projectile Creates Rapid Changes in Pressure & Temperature that Propagate Through Tissue Causing Additional Injury
Blunt Mechanisms:
Crushing Force – Direct Compression Causing Injury
Shearing Force – Tearing from Acceleration/Deceleration Around Fixed Attachments
Bursting Force – Force Causing Acutely Increased Intraluminal Pressure within Hollow Organs Leading to Rupture
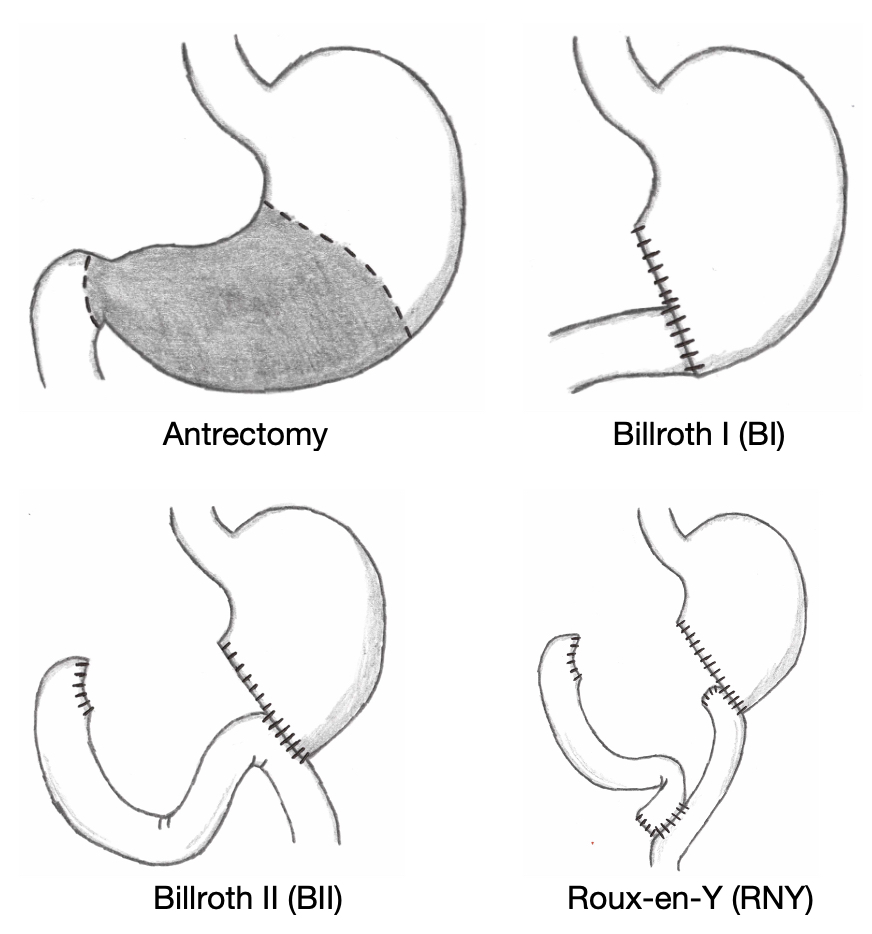
Significant Tissue Loss/Devascularization: Partial Gastrectomy and Reconstruction (Billroth I/II vs. Roux-en-Y)
If Too Severe to Reconstruct: Total Gastrectomy and Roux-en-Y Esophagojejunostomy
Delay to Surgery with Perforation is Associated with Increased Morbidity and Mortality
Reconstruction After Partial Gastrectomy
References
Angelopoulos S, Mantzoros I, Kyziridis D, Fontalis A, Parpoudi S, Konstandaras D, Tsalis C. A rare case of a transabdominal impalement after a fall from a ladder. Int J Surg Case Rep. 2016;22:40-3. (License: CC BY-NC-ND-4.0)