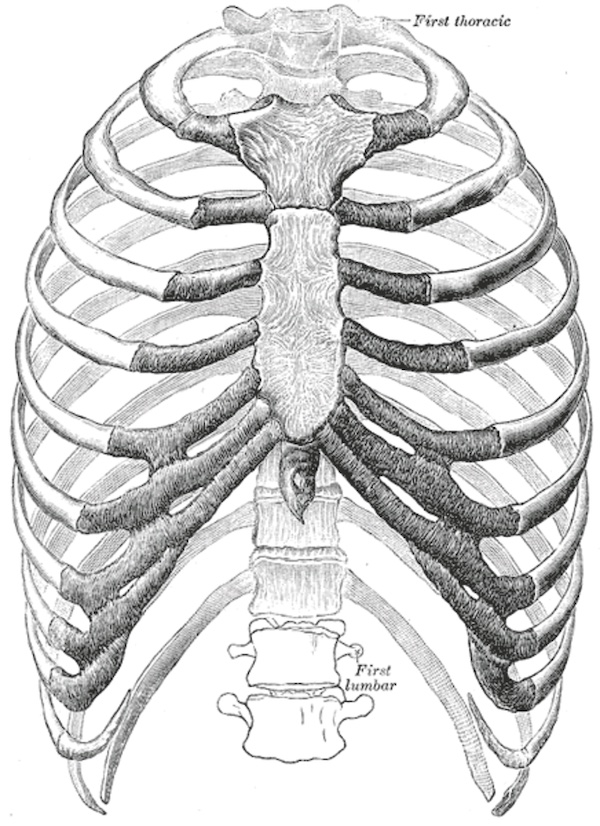
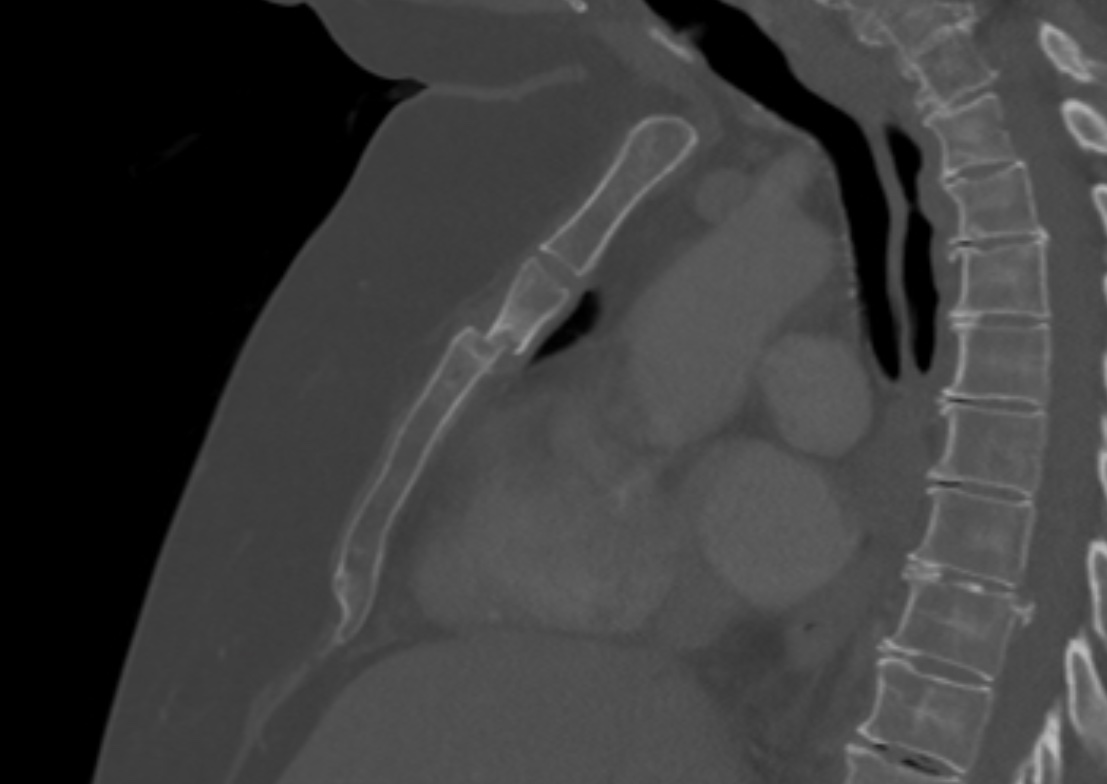
Sternal Fracture Sternal Fracture David Ray Velez, MD Table of Contents BackgroundPresentation and DiagnosisTreatmentSee Also:*See Blunt Cardiac Injury (BCI) Background AnatomyManubrium – Upper Quadrangular PortionJoins the Clavicle and Upper 1.5 RibsBody (Gladiolus) – Middle Longest PortionAttachment of the Pectoralis MajorArticulates with the Majority of the True RibsXiphoid Process – Inferior TipFracture SiteBody: 55.8% – Most CommonManubrium: 31.7%Body and Manubrium: 12.5%Most Commonly Caused by Blunt Anterior Chest Wall Trauma and Deceleration InjuriesMotor Vehicle Crash (MVC) is the Most Common Cause (68%) – Increased Incidence Since the Introduction of Seat Belt Laws Requiring Shoulder RestraintsCan Be Caused by Cardiopulmonary Resuscitation (CPR) – 18% Incidence in One Autopsy-Based StudyMortalityIsolated Sternal Fracture: 0.4-3.5%Polytrauma: 3.8-10.4% Sternum Presentation and Diagnosis Significant Force Required to Fracture and the Majority (73.6%) Have Polytrauma with Multiple InjuriesMost Common Associated InjuriesRib Fracture (57.8%) – Most CommonLung Contusion (33.7%)Pneumothorax (22.0%)Vertebral Fracture (21.6%)Lumbar Vertebrae Fracture (16.9%)Concussion (3.9%)Blunt Cardiac Injury (3.6%)Sternal Fracture Alone Does Not Predict the Presence of Blunt Cardiac Injury (BCI) – Previously Believed to Be – *See Blunt Cardiac Injury (BCI)PresentationChest Pain – Worse with Movement, Deep Breathing, or CoughClicking Sensation with MovementShortness of BreathSwelling or EcchymosisPalpable Deformity or CrepitusDiagnosisCT is the Standard Diagnostic EvaluationGenerally Best Seen on Sagittal Imaging and May Be Missed if Looking at Axial Images AloneChest X-Ray Has Low SensitivityAP: 50%Lateral: 70%US Has Similar Sensitivity to Plain Radiography Sternal Fracture Treatment Primarily Treated by Nonoperative ManagementMultimodal Analgesia – *See Multimodal AnalgesiaPulmonary Hygiene – *See Pulmonary Hygiene (Pulmonary Toilet)Most Isolated Sternal Fractures Heal Spontaneously with Pain Lasting an Average of 10.9 WeeksSurgical Stabilization (Open Reduction and Internal Fixation/ORIF)Rarely PerformedIndications for Surgical Stabilization are Poorly Established Compared to Rib FracturesPotential Indications:Visible DeformityLoss of Sternal ContinuityComplete DisplacementSternomanubrial Joint Dislocation/FracturePersistent Mobility/ClickingUncontrolled PainChronic Pain or NonunionGenerally Performed Using Titanium Plates