
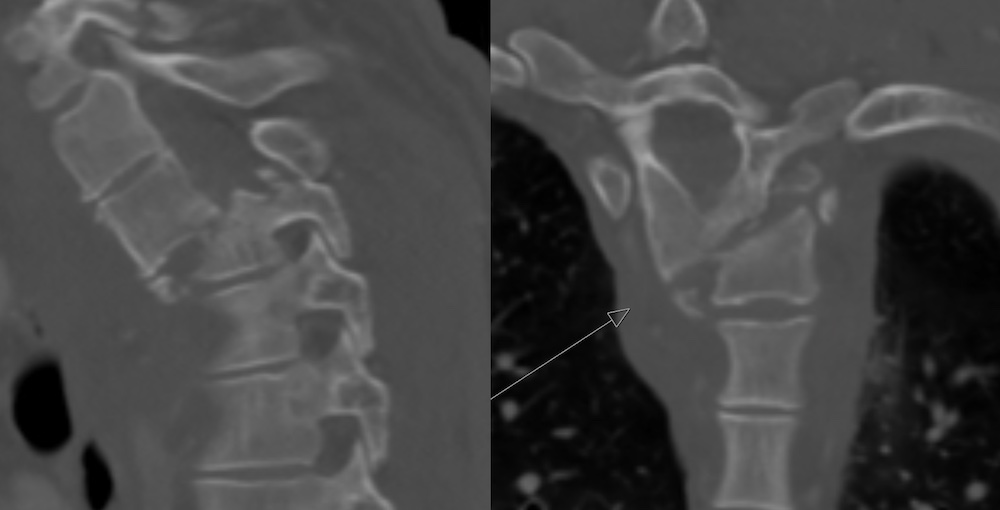
Thoracic (Left) and Lumbar (Right) Vertebrae
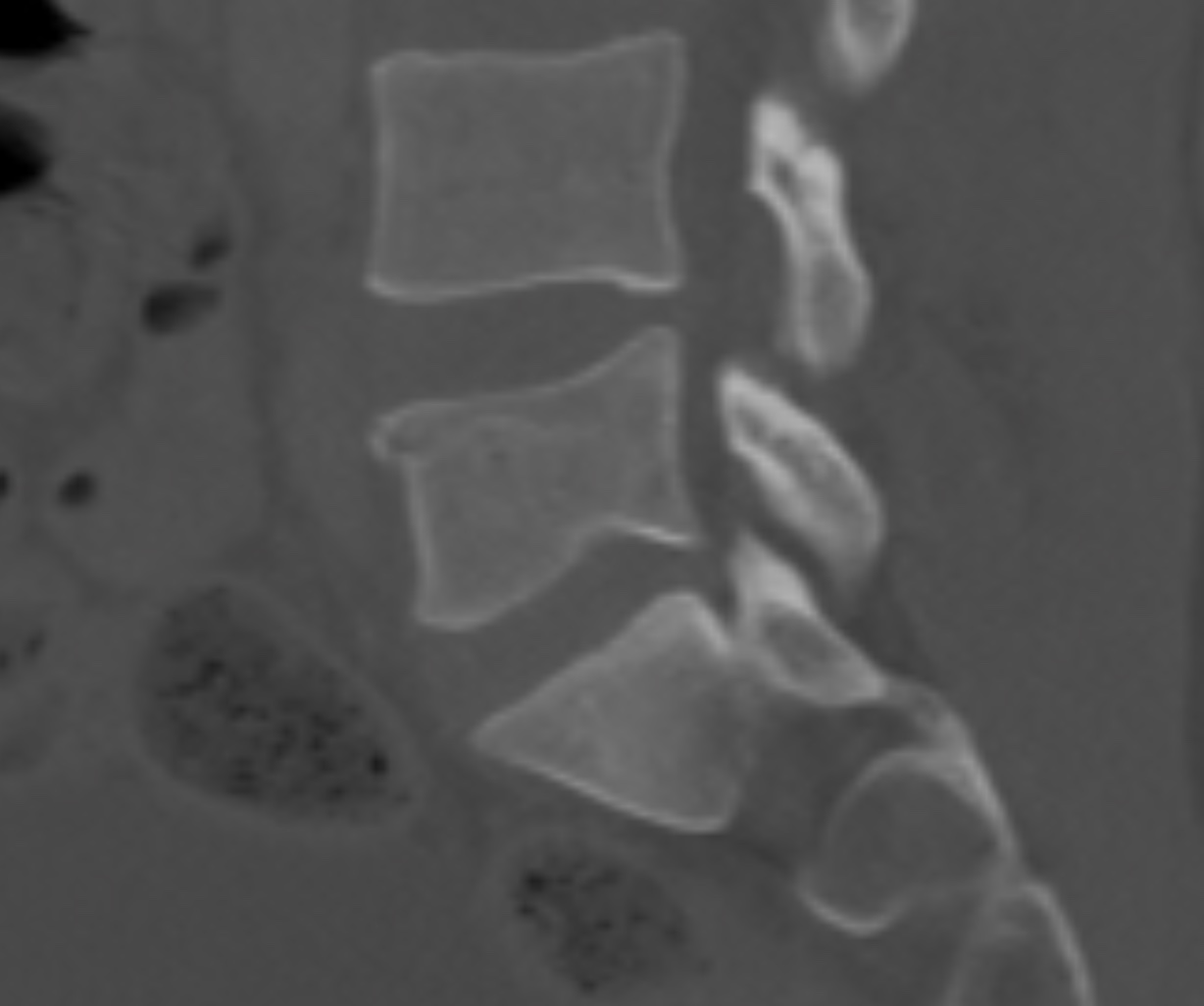
Wedge (Compression) Fracture

Burst Fracture
Chance Fracture
![]()
Transverse Process Fracture

Spinous Process Fracture
Thoracic (Left) and Lumbar (Right) Vertebrae
Wedge (Compression) Fracture
Burst Fracture
Chance Fracture
![]()
Transverse Process Fracture
Spinous Process Fracture