Rib Fracture
Rib Fracture
David Ray Velez, MD
Table of Contents
Anatomy
Anatomy
- 12 Ribs on Each Side
- True Ribs (#1-7): Attach Directly to the Sternum by Costal Cartilage
- False Ribs (#8-12): Do Not Attach Directly to the Sternum by Costal Cartilage
- Costal Cartilage of Ribs #8-10 Unite Before Indirectly Attaching to the Sternum
- Floating Ribs (#11-12): Do Not Attach at All
Fracture
- Ribs #1-3 are the Most Difficult to Fracture and Require Significant Force
- Ribs #4-10 are the Most Commonly Fractured
- Ribs #11-12 are Mobile and More Difficult to Fracture
Pediatrics Have More Elastic Ribs than Adults and are Less Vulnerable to Rib Fracture
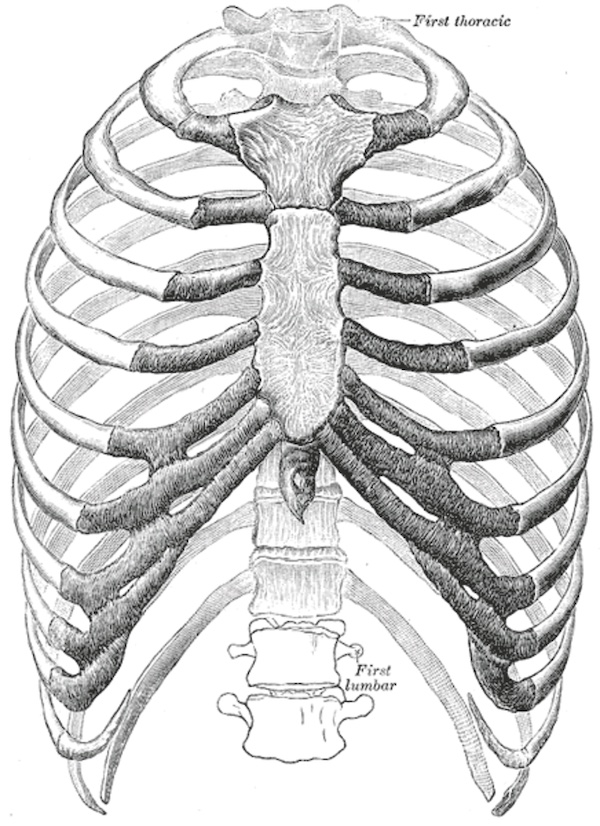
Rib Cage
Presentation and Complications
Presentation
- Severe Pain – Worse with Deep Breathing and Movement
- Shortness of Breath/Dyspnea
- Clicking Sensation with Movement
- Swelling or Ecchymosis
- Palpable Deformity or Crepitus
Respiratory Splinting
- Definition: Reduced Inspiratory Effort Due to Severe Pleuritic Chest Pain or Fear of Pain Upon Inspiration
- Patients Therefore Only Take Rapid Shallow Breaths
- Expiration – A Passive Process that Relies on the Elastic Recoil of the Lung
- Inspiration – An Active Process that Requires Muscular Contraction
- Results In:
- Hypoventilation
- Atelectasis
- Pneumonia
- Retained Secretions
- Respiratory Failure
- Can Quantify Dynamically with Incentive Spirometry (IS)
- Goal: > 15 cc/kg Ideal Body Weight
Complications
- Pulmonary Contusion – *See Pulmonary Injury
- Initial CXR Underestimates and Worsens with Time and Fluid Resuscitation
- Atelectasis – *See Atelectasis
- Pneumonia (PNA)
- Acute Respiratory Distress Syndrome (ARDS)
- Respiratory Failure
- Pneumothorax (PTX) – *See Pneumothorax (PTX)
- Hemothorax (HTX) – *See Hemothorax (HTX)
- Injury to Internal Organs – Heart, Spleen, Liver, Kidney, etc.
- Chronic Pain
- Significantly Increased Mortality
Morbidity and Mortality Significantly Increase Once > 6 Rib Fractures
Elderly
- Rib Fractures are the Most Common Injury in the Elderly After Blunt Chest Trauma
- Each Additional Rib Fracture Increases:
- Risk of Death by 19%
- Risk of Pneumonia by 27%
- *Risk May Be Overestimated by Older Studies without Modern Imaging
Description/Definition
Complexity
- Simple: Single Fracture Line Across the Rib with No Fragmentation or Comminution
- Wedge: A Second Fracture Line that Does Not Span the Entire Rib Width
- Complex: ≥ 2 Fracture Lines with ≥ 1 Fragment Spanning the Entire Rib Width
Displacement
- Nondisplaced: ≥ 90% of the Fracture Cortical Surfaces are in Contact
- Offset: Some Cortical Contact But < 90% of the Fracture Cortical Surfaces are in Contact
- Displaced: No Cortical Contact Between Fracture Surfaces
Location/Area
- Anterior: Anterior to the Anterior Axillary Line
- Lateral: Between the Anterior & Posterior Axillary Lines
- Posterior: Posterior to the Posterior Axillary Line
Flail Chest
- Definitions:
- Flail Segment: ≥ 3 Adjacent Ribs Fractured in ≥ 2 Places
- *Some Texts Say ≥ 2 Adjacent Ribs Fractured in ≥ 2 Places
- Flail Chest: Flail Segment with the Clinical Paradoxical Chest Wall Movement
- Flail Segment: ≥ 3 Adjacent Ribs Fractured in ≥ 2 Places
- Paradoxical Breathing: The Fractured Segment is Pulled Inward with Inhalation and Outward with Exhalation
- Disrupts Normal Respiratory Mechanics
- Collapse Causes Air Movement from the Injured Lung to the Uninjured Lung – Results in a Possible Mediastinal Shift to the Injured Side
- Risk for Underlying Pulmonary Contusion
- Initial CXR Underestimates and Worsens with Time and Fluid Resuscitation
Flail Chest 1
Diagnosis
Chest X-Ray (CXR)
- CXR is Generally the Initial Imaging Modality After Chest Wall Trauma
- Can Rapidly Evaluate for Other Life-Threatening Injuries (HTX/PTX)
- Poor Sensitivity for Rib Fractures (33-40%) – Often Underestimates or Completely Misses
Chest CT
- The Gold Standard for Rib Fracture Diagnosis
- Identifies Significantly More Fractures and Thoracic Injuries than CXR
- Over Half of Patients with Rib Fracture Find ≥ 3 More Rib Fractures on CT than CXR
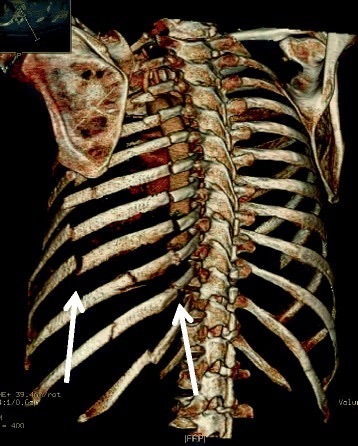
Can Obtain 3D Reconstructions of Chest CT to Better Evaluate and Plan Surgical Intervention – Their Routine Use, However, Has Not Been Shown to Change Management or Improve Outcomes
Classification Systems
RibScore
- The Most Extensively Validated Scoring System
- Based on Static Radiographic Data
- Factors:
- ≥ 6 Fractures
- Bilateral Fractures
- Flail Chest
- ≥ 6 Severely (Bicortical) Displaced Fractures
- First Rib Fracture
- ≥ 1 Fracture in All Three Anatomic Areas (Anterior, Lateral, and Posterior)
- Scores ≥ 4 Have Higher Risk for Pulmonary Complications (Pneumonia, Respiratory Failure, and Tracheostomy)
Sequential Clinical Assessment of Respiratory Failure (SCARF) Score
- A Dynamic Physiologic Score Measured Daily
- Factors:
- Number Pain Score ≥ 5
- Incentive Spirometry < 50% Predicted
- Respiratory Rate ≥ 20
- Poor Cough
- Interpretation:
- Score 0: Low Risk of Adverse Outcomes
- Score 1-2: Intermediate Risk of Adverse Outcomes
- Score 3-4: High Risk of Adverse Outcomes
- Scores > 2 After Interventions Should Prompt Consideration for Increasing Analgesia Regimen
Rib Injury Guideline (RIG)
- A Scoring System Used to Guide Admission/Disposition
- Factors:
- Age ≥ 60 Years – 4 Points
- IS < 750 mL – 4 Points
- Severe Pulmonary Contusions on CT – 2 Points
- Fractures ≥ 5 – 2 Points
- COPD, Asthma, or Smoker – 2 Points
- HTX, PTX, or Chest Tube Placed – 2 Points
- Pain Score ≥ 6/10 – 1 Point
- Weak or Absent Cough – 1 Point
- Interpretation:
- RIG 1 (Score ≤ 2): Discharge if Possible
- RIG 2 (Score 3-9): Floor Admission
- RIG 3 (Score ≥ 10 or Severe Extra-Thoracic Injury): ICU Admission
Other Scoring Systems
- AAST Organ Injury Scale (OIS)
- Rib Fracture Score (RFS)
- Chest Trauma Score (CTS)
- Thoracic Trauma Severity Score (TTSS)
- Battle Score
- Revised Intensity Battle Score (RIBS)
Treatment
Primarily Treated by Nonoperative Management
- Multimodal Analgesia – *See Multimodal Analgesia
- Pulmonary Hygiene – *See Pulmonary Hygiene (Pulmonary Toilet)
Consider ICU Admission for All Elderly Patients with Significant Fractures
Surgical Stabilization of Rib Fractures (SSRF)
- Also Known as: Rib Plating or Open Reduction and Internal Fixation (ORIF) of the Ribs
- The Use and Exact Indications for SSRF is Highly Debated and Evolving
- Early Timing is Preferred as Prolonged Trials (7-10 Days) of Nonoperative Management for Multiple Displaced Rib Fractures Increases the Risk of Pulmonary Compromise
- Potential Indications:
- Flail Segment with Respiratory Failure or Poor Response to Nonoperative Management
- Multiple Displaced Rib Fractures
- Nonunion
- Significant Deformity
- Refractory Pain
- Unable to Wean Off Ventilator
- During Thoracotomy for Other Indication – “On the Way Out”
- Generally Only Plate Ribs #4-9 – Where the Majority of Chest Wall Movement Occurs
- Ribs #1-3 Have Little Movement and Are Difficult to Access
- Ribs #10-12 Add Little to Chest Wall Stability
Pulmonary Contusion is Not a Contraindication to SSRF – Early Reports Advocated Against but Newer Data Shows Favorable Outcomes
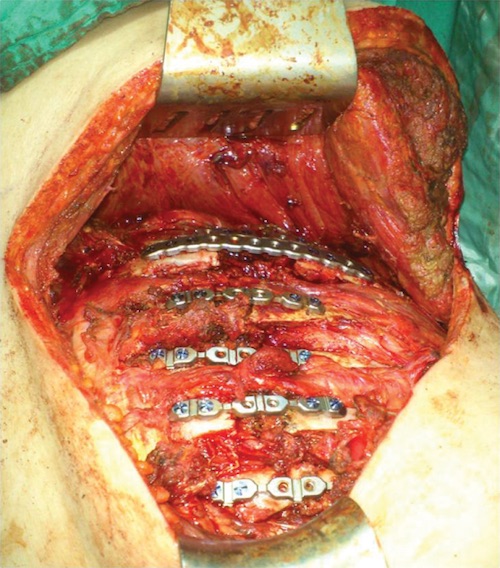
Rib Plating 2
References
- Granhed HP, Pazooki D. A feasibility study of 60 consecutive patients operated for unstable thoracic cage. J Trauma Manag Outcomes. 2014 Dec 30;8(1):20. (License: CC BY-2.0)
- Evman S, Kolbas I, Dogruyol T, Tezel C. A Case of Traumatic Flail Chest Requiring Stabilization with Surgical Reconstruction. Thorac Cardiovasc Surg Rep. 2015 Dec;4(1):8-10. (License: CC BY-NC-SA-4.0)