*The Classic Triad is Rare and Only Seen in < 10% of Patients
Additional Symptoms
Lethargy
Tachycardia
Fever
Nausea/Vomiting
Abdominal Pain
Altered Mental Status
Complications
Acute Kidney Injury (AKI)
The Most Significant Complication
From Hypovolemia and Nephrotoxic Myoglobin
Risk: 10-40%
Compartment Syndrome
Hypovolemia – From Fluid Accumulation within the Damaged Muscle
Hyperkalemia
Hyperphosphatemia
From Hyperphosphatemia and Calcium Deposition in Damaged Muscle
Disseminated Intravascular Coagulation (DIC)
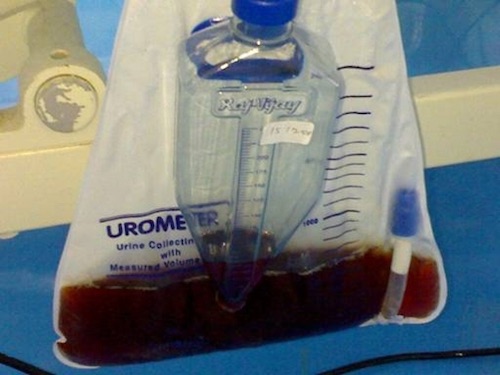
Tea-Colored Urine of Rhabdomyolysis 1
Diagnosis
Labs
Elevated Creatinine Kinase (CK)
Myoglobinuria
Electrolyte Disturbances:
Hyperkalemia – Released from Damaged Cells
Hyperphosphatemia – Released from Damaged Cells
Hypocalcemia (Early) – Calcium Initially Enters into the Damaged Myocytes
Hypercalcemia (Late) – Calcium within the Damaged Cells Eventually Efflux Out
Anion Gap Metabolic Acidosis
High Uric Acid
Clinical Diagnosis
Diagnosis: Acute CK Elevation with Either Clinical Signs (Weakness/Dark Urine) or Myoglobinuria on UA
CK > 5,000 U/L is Often Used but No Absolute Cutoff is Defined
Treatment
Correct Any Underlying Pathology (Fasciotomy, etc.)
Primary Treatment: Aggressive IV Fluid Resuscitation (LR or NS)
Goal Urine Output: 1-3 mL/kg/hr
The Primary Goal of Fluid Resuscitation is to Prevent AKI
May Require Dialysis for Volume Overload, Acidemia, Hyperkalemia, or Uremia
Generally Avoid Mannitol or Diuretics
Sodium Bicarbonate
Goal: Urinary Alkalinization to Prevent Cast Formation
Use is Poorly Defined and Controversial
Does Not Reduce the Risk of AKI or Mortality
Contraindications:
Hypocalcemia – May Worsen
pH ≥ 7.5
HCO3 ≥ 30
References
Ganeshram P, Goundan PN, Jeyachandran V, Arthur P. Five factors contributing to severe rhabdomyolysis in a 21 yr old IV drug abuser: a case report. Cases J. 2009 Jul 7;2:6479. (License: CC BY-3.0)
The most high-yield and effective guide to master mechanical ventilation. An essential resource for students, trainees, and clinicians. This is the review book you will actually use!