May Consider Primary Repair for Even Destructive Rectal Injuries if Feasible and Not Requiring Significant Blood Transfusion or Hemodynamically Unstable
Diversion (Ostomy) Indications
Significant Blood Transfusion (> 4-6 Units)
Shock on Vasopressor Support
*Fecal Contamination Alone is Associated with Increased Risk of Abscess but Not Anastomotic Failure and Should Not Be Used as an Indication for Colostomy (Nor is Location or Associated Abdominal Injuries)
Extraperitoneal Injury – Treatment
Accessible: Primary Repair Through a Transanal Approach
Transanal Minimally Invasive Surgery (TAMIS) if Able
Diverting Colostomy if Requiring Significant Blood Transfusion or Hemodynamically Unstable
Inaccessible: Diverting Colostomy
Loop Sigmoid Colostomy is Generally Preferred
End Colostomy Considered for Devastating Injuries
Can Take Down in 6-8 Weeks
Historical Considerations
Presacral Drainage (Previously Recommended for Extraperitoneal Injuries) is Inadequate and Should Not Be Pursued
Distal Rectal Washout is Outdated and May Actually Increase the Risk of Infectious Complications
References
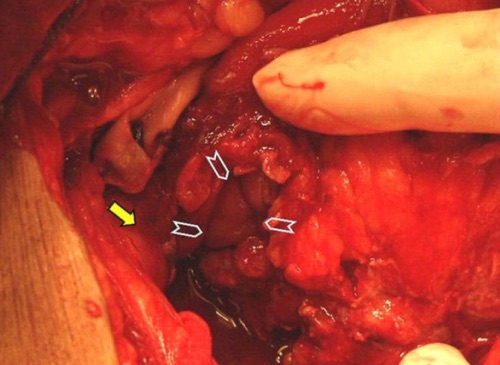
Hefny AF, Al-Ashaal YI, Bani-Hashem AM, Abu-Zidan FM. Seatbelt syndrome associated with an isolated rectal injury: case report. World J Emerg Surg. 2010 Feb 4;5(1):4. (License: CC BY-2.0)
Coskun A, Erkan N, Yakan S, Yıldirim M, Cengiz F. Management of rectal foreign bodies. World J Emerg Surg. 2013 Mar 13;8(1):11. (License: CC BY-2.0)
Hefny AF, Salim EA, Bashir MO, Abu-Zidan FM. An unusual stab wound to the buttock. J Emerg Trauma Shock. 2013 Oct;6(4):298-300. (License: CC BY-NC-SA-3.0)