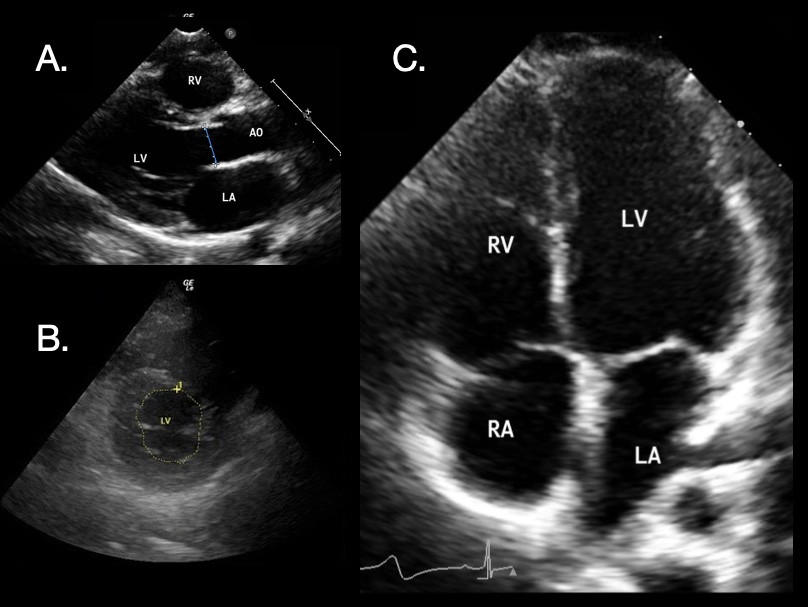
Cardiac POCUS: (A) Parasternal Long-Axis 1; (B) Parasternal Short-Axis 2; (C) Apical 4-Chamber 1 [Right Atrium (RA), Right Ventricle (RV), Left Atrium (LA), Left Ventricle (LV), Aortic Outflow (AO)]
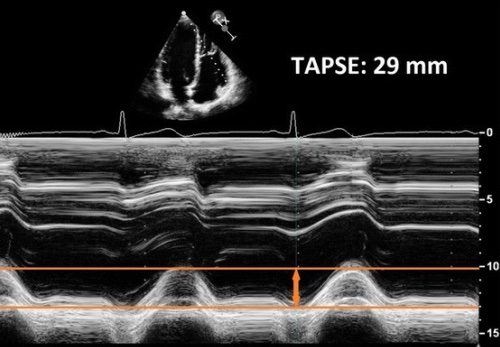
TAPSE on POCUS 3
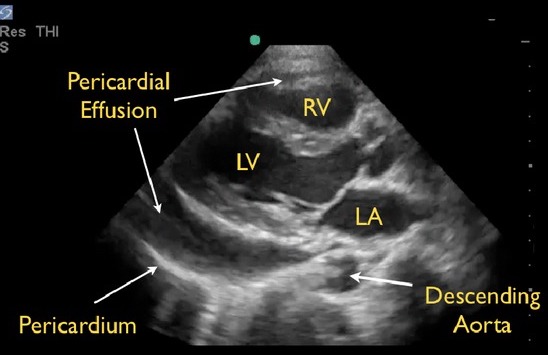
Pericardial Effusion on POCUS: Anterior to the Descending Aorta 4
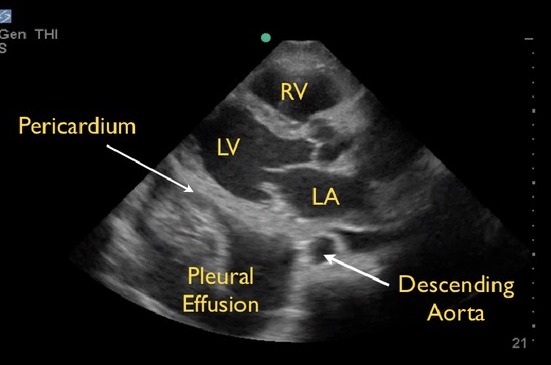
Pleural Effusion on POCUS: Posterior to the Descending Aorta 4
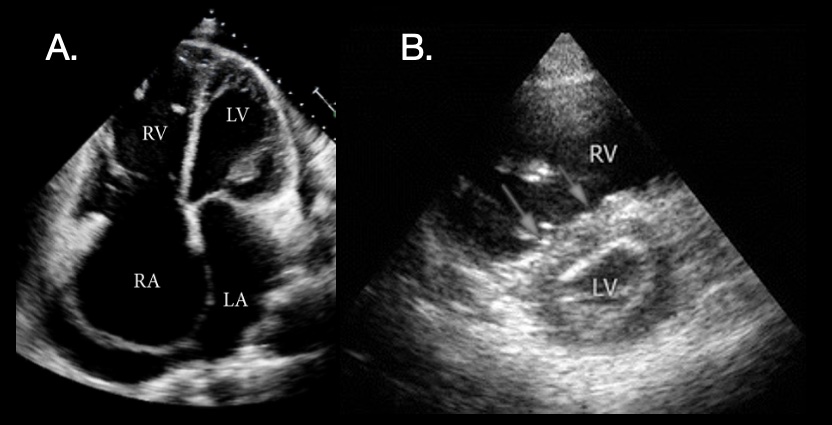
PE POCUS: (A) Significant Right-Sided Distention 1; (B) “D-Sign” on Short-Axis View with Dilated RV, Flattened Septum (Arrows), and D-Shape of LV 2
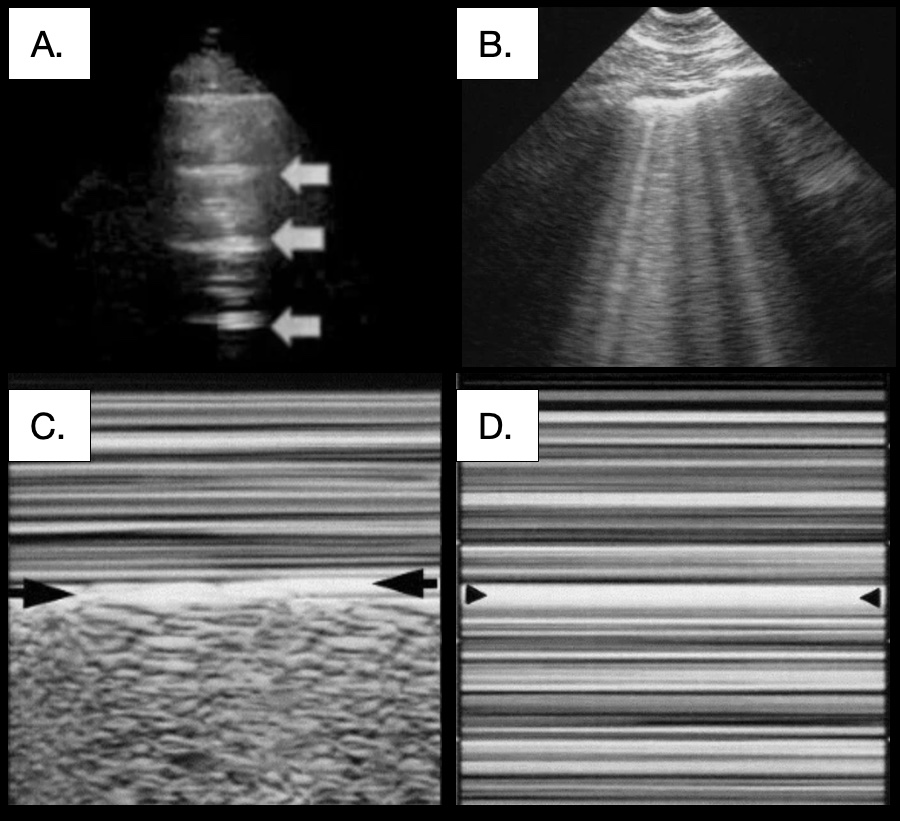 Pulmonary POCUS: (A) A-Lines (Arrows) 5; (B) B-Lines 6; (C) Seashore Sign 6; (D) Barcode Sign 6
Pulmonary POCUS: (A) A-Lines (Arrows) 5; (B) B-Lines 6; (C) Seashore Sign 6; (D) Barcode Sign 6 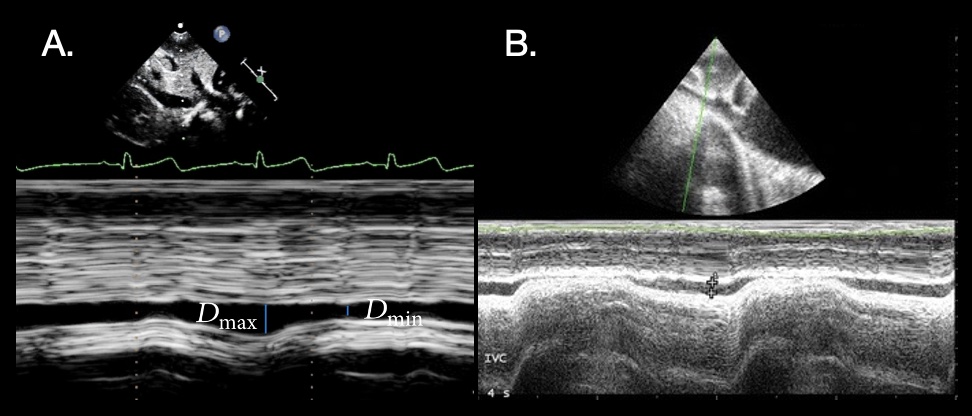
IVC Collapsibility POCUS: (A) Normal 1; (B) Collapse 2

