
Minimum Equipment for Pericardiocentesis: Large 18 Gauge Spinal Needle and Syringe
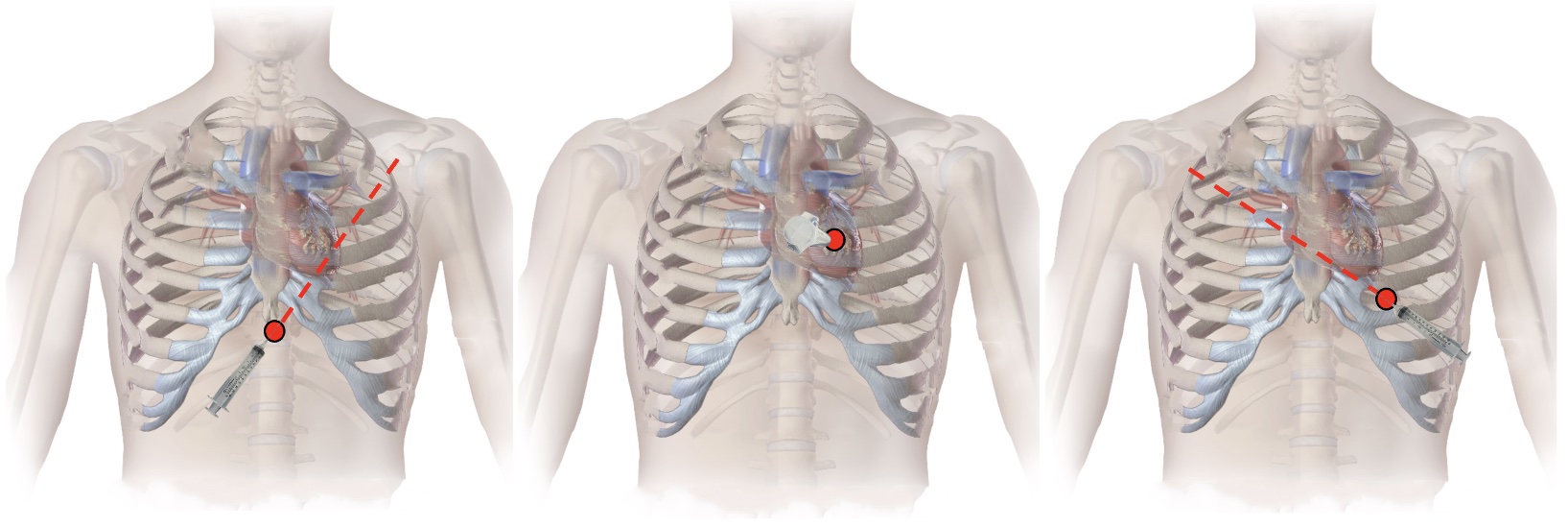
Pericardiocentesis Approaches: Subxiphoid (Left), Parasternal (Middle), and Apical (Right) 2
Minimum Equipment for Pericardiocentesis: Large 18 Gauge Spinal Needle and Syringe
Pericardiocentesis Approaches: Subxiphoid (Left), Parasternal (Middle), and Apical (Right) 2

