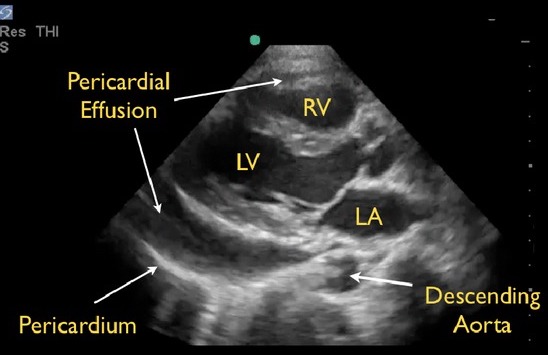
Pericardial Effusion on POCUS: Anterior to the Descending Aorta 2
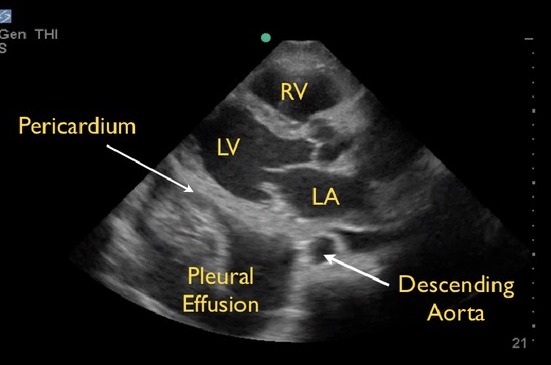
Pleural Effusion on POCUS: Posterior to the Descending Aorta 2
Pericardial Effusion on POCUS: Anterior to the Descending Aorta 2
Pleural Effusion on POCUS: Posterior to the Descending Aorta 2

