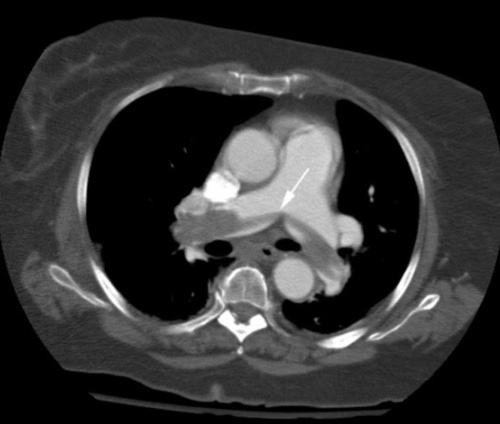
Saddle Pulmonary Embolism on CTA 1
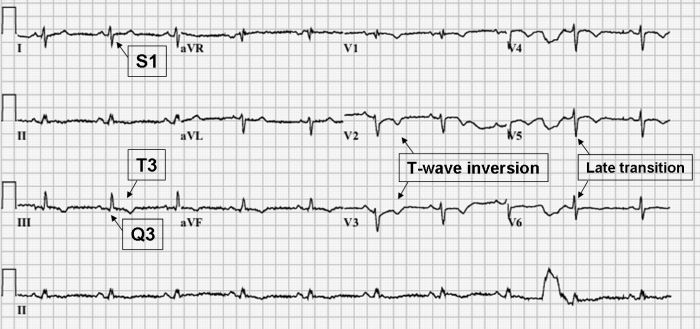
S1Q3T3 on EKG 2
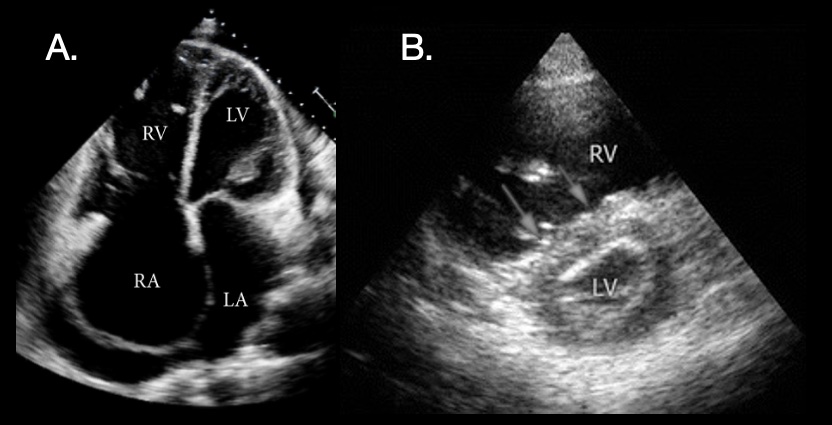
PE POCUS: (A) Significant Right-Sided Distention; (B) “D-Sign” on Short-Axis View with Dilated RV, Flattened Septum (Arrows), and D-Shape of LV 3,4
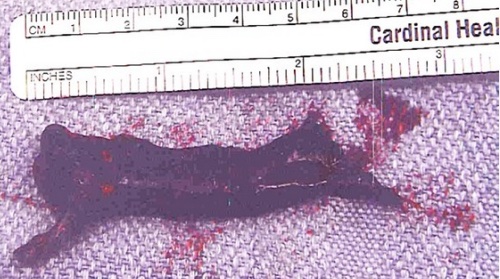
Pulmonary Embolism Removed by Thrombectomy 5
Saddle Pulmonary Embolism on CTA 1
S1Q3T3 on EKG 2
PE POCUS: (A) Significant Right-Sided Distention; (B) “D-Sign” on Short-Axis View with Dilated RV, Flattened Septum (Arrows), and D-Shape of LV 3,4
Pulmonary Embolism Removed by Thrombectomy 5