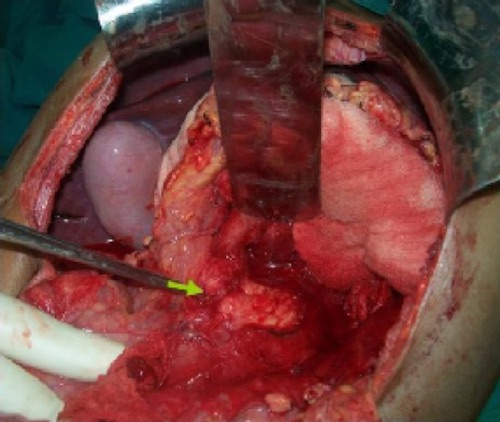
Pancreatic Neck Laceration 1
![]()
Pancreatic Duct Transection on MRCP 2

Distal Pancreatectomy and Splenectomy 3
MNEMONIC: “Treat the Pancreas Like a Crawfish”
- Suck (Drain) the Head
- Eat (Resect) the Tail
Pancreatic Neck Laceration 1
![]()
Pancreatic Duct Transection on MRCP 2
Distal Pancreatectomy and Splenectomy 3
MNEMONIC: “Treat the Pancreas Like a Crawfish”