
Laryngeal Anatomy and Target Site for Percutaneous Cricothyroidotomy (Red Circle)
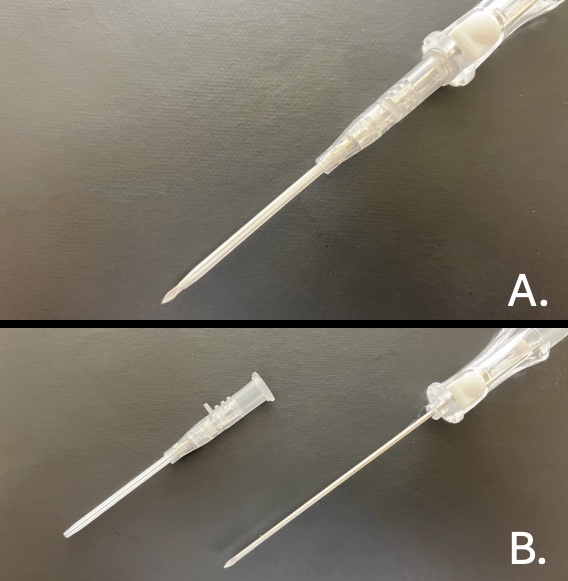
16 Guage Angiocatheter
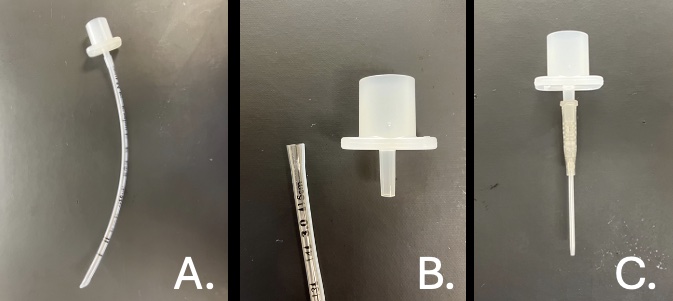
Endotracheal Tube Adaptor (ETTA): 3-0 Endotracheal Tube (A), ETTA Disconnected (B), ETTA Attached to Catheter (C)
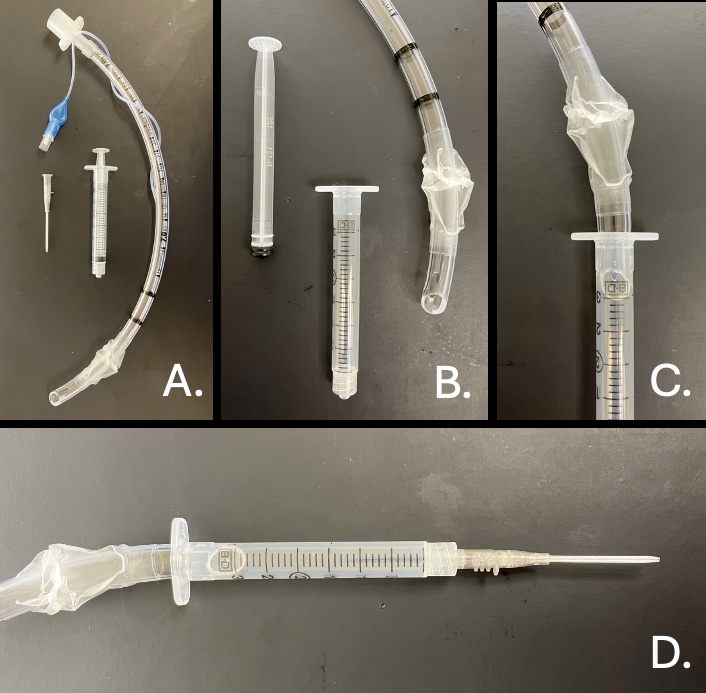
Connection Using a 3 mL Syringe and 7-0 ETT
Connection Using a 10 mL Syringe and 7-0 ETT – Cuff Inflated
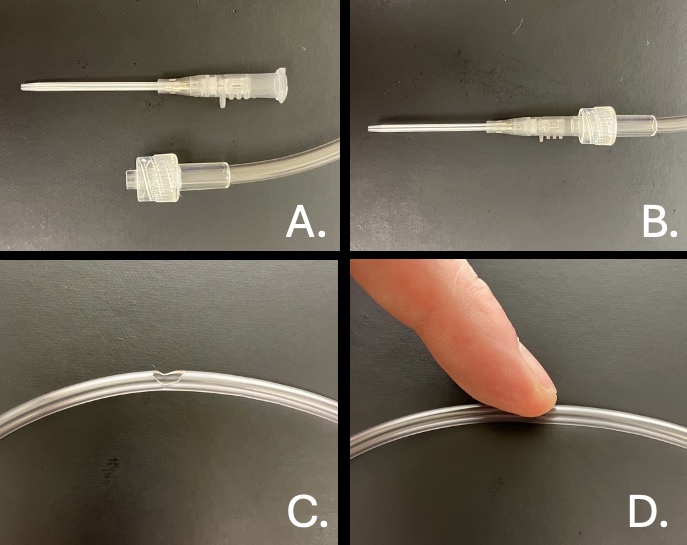
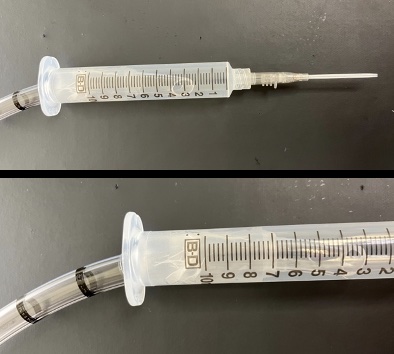
Jet Ventilation by Direct Attachment: Release/Ventilation (C), Occlude/Oxygenation (D)
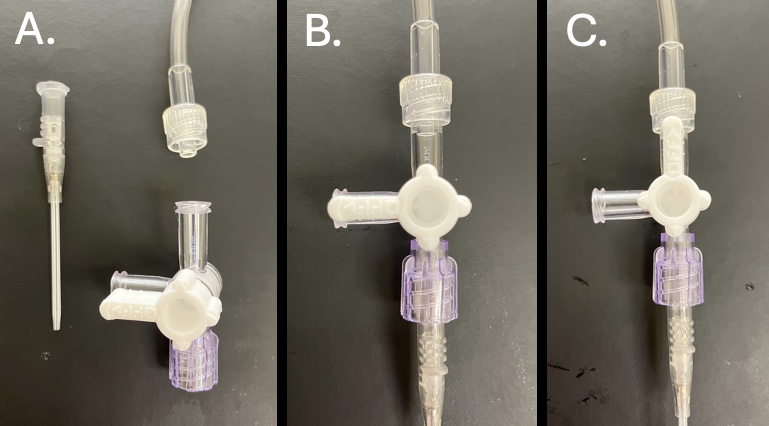
Jet Ventilation with a 3-Way Stopcock: Occlude/Oxygenation (B), Release/Ventilation (C)

