Neck Exploration
Neck Exploration
David Ray Velez, MD
Table of Contents
Neck Exploration
Definitive Management
Exploring the Wounded Neck is a “Safari in Tiger Country” Per “Top Knife” by Hirshberg & Mattox
Neck Exploration
Positioning
- Supine
- Arms Tucked at Side
- Neck Fully Extended with a Shoulder Roll and Rotated to the Contralateral Side
Incision
- Longitudinal Incision Along the Anterior/Medial Border of the Sternocleidomastoid (SCM) Muscle
- Can Extend the Incision as Needed from the Mastoid Process to the Sternal Notch
- Can Extend Exposure with a “U”-Incision for Transcervical Injuries – Bilateral Incisions Along the SCM Muscles Meeting at the Bottom and Lifting a Subplatysmal Flap Up
“Trail of Safety”
- Step 1. Sternocleidomastoid (SCM) Muscle
- Divide the Platysma – The First Layer Seen Beneath the Skin
- Expose the Anterior Border of the Sternocleidomastoid (SCM) Muscle
- Step 2. Internal Jugular (IJ) Vein
- Retract the SCM Laterally to Expose the Working Area
- Dissect Through the Middle Cervical Fascia Until the IJ is Identified
- The IJ is the Most Commonly Injured Vascular Structure in Neck Exploration
- Step 3. Facial Vein
- Described as the “Gatekeeper” to the Neck
- Identify and Ligate the Fascial Vein – Seen Crossing Medially from the IJ
- There May Be More Than One Small Vein That Requires Ligation
- Ligation Allows Mobilization of the IJ for Exploration of Deeper Structures
- Step 4. Carotid Artery
- Retract the IJ Laterally
- Enter the Carotid Sheath and Identify the Carotid Artery
- Identify and Protect the Vagus Nerve – Generally Lies Between the IJ and Carotid
Obtain Both Proximal and Distal Vascular Control in Virgin Territory Before Entering a Hematoma
- For More Proximal Control: Median Sternotomy
- For More Distal Control: May Require Mandible Disarticulation
- Control at the Bifurcation Includes Control of the Common Carotid Artery (CCA), Internal Carotid Artery (ICA), and External Carotid Artery (ECA)
Esophagus Exploration
- Left Cervical Incisions are Preferred for Esophageal Exploration if Able
- The Esophagus is Slightly Left of Midline
- The Left Recurrent Laryngeal Nerve is Longer and More Vertical than Right – Less Likely to Be Injured
- Explore the Esophagus by Dissecting Medial to the Carotid Sheath
- Alternatively, Can Explore the Esophagus Posterior to the Carotid Sheath by Retracting the Sheath Medially – More Limited Exposure
- The Esophagus Will Be Posterior to the Trachea and Anterior to the Spine
- Have Anesthesia Place a Large-Bore Orogastric (OG) Tube to Assist in Palpation/Identification
- Exposure May Require Division of the Omohyoid Muscle, Middle Thyroid Vein, and Inferior Thyroid Artery
- Take Caution to Avoid Injury to the Recurrent Laryngeal Nerve – Travels in the Tracheoesophageal Groove

Neck Incisions
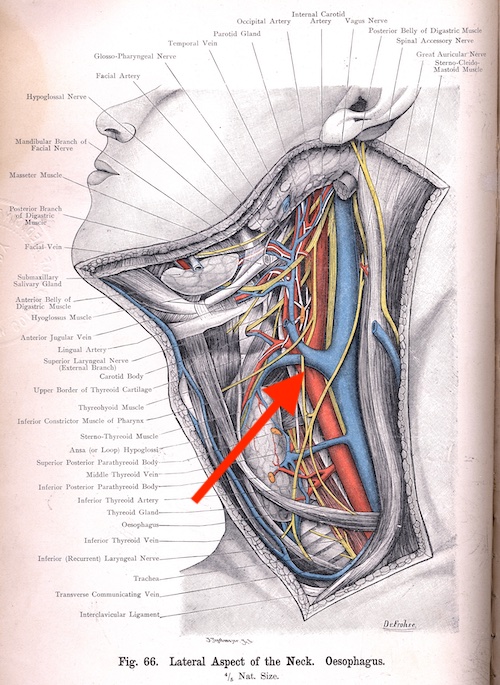
Facial Vein
Definitive Management
Vascular Injury
Larynx/Trachea Injury
Esophagus Injury