Morel-Lavallee Lesion
Morel-Lavallee Lesion
David Ray Velez, MD
Table of Contents
Definition and Pathophysiology
Definition: Closed Degloving Soft Tissue Injury Causing Dermal-Fascial Separation
Pathophysiology
- Skin and Subcutaneous Tissue are Separated from the Underlying Fascia
- Shear Injury Causes Disruption of Blood Vessels and Lymphatics
- Creating a Space for Fluid Collection
4-Stages
- Stage 1: Shearing Force Causes Dermal-Fascial Separation
- Stage 2: Fluid is Produced from Injured Blood Vessels and Lymphatics
- Stage 3: Fluid is Replaced by Serosanguinous Fluid Over Time
- Stage 4: Local Inflammation Causes a Pseudocapsule Formation
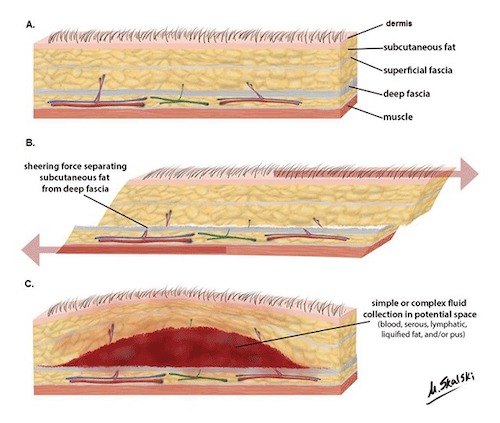
Morel-Lavalle Lesion – Mechanism of Injury 1
Presentation
Presentation
- Classic Presentation: Enlarging Painful Lesion with Swelling and Fluctuance
- Ecchymosis with Pain Out-of-Proportion
- High Risk for Infection – 46% Have Bacterial Colonization
- High Risk for Skin Necrosis
Up to 33% are Missed on the Initial Examination
Locations
- Peri-Trochanter Region of Proximal Thigh – Most Common Site
- Buttock
- Back
- Abdomen
- Flank
Most Common Etiology: Motor Vehicle Crash (MVC)

Morel-Lavallee Lesion – Skin Necrosis on Day #4 2
Diagnosis and Classification
Diagnosis Requires a High Index of Suspicion
Diagnosis – Primarily Based Upon Imaging
- CT – Most Common
- MRI (Preferred in Some Literature and Generally Considered the Gold Standard for Chronic Lesions)
- May Be Seen on US but Less Common
Classification (Mallado and Bencardino)
- *Largely Based on MRI Findings
- Type I: Seroma
- Type II: Subacute Hematoma
- Type III: Chronic Organizing Hematoma
- Type IV: Perifascial Dissection with Closed Fatty Laceration
- Type V: Perifascial Pseudonodular Lesion
- Type VI: Infected Lesion
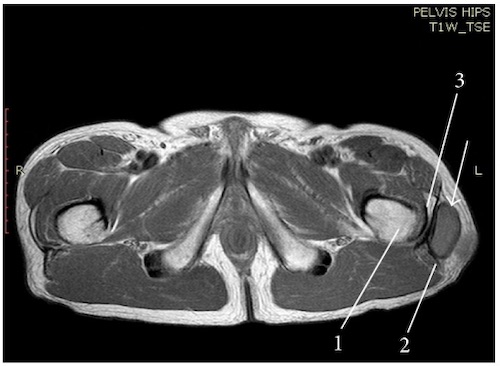
Morel-Lavallee Lesion of Left Hip on MRI 3
Treatment
Acute Lesions
- Small (< 50 mL) and Asymptomatic: Compression (ACE Wrap or Compressive Bandages)
- Also Consider Needle Aspiration
- Large (> 50 mL) or Symptomatic: Percutaneous Drainage
- Infected Lesions Require Early Debridement and Wound Care
Chronic/Encapsulated Lesions
- Primary Treatment is Incision & Drainage
- Any Pseudocapsule Should be Resected to Decrease the Recurrence Risk
- Necrotic Skin Requires Debridement and Possibly Skin Grafting
- Exact Surgical Approach is Poorly Defined – May Consider WVAC, Retention Sutures of Fascia to Skin, etc.
- Other Options:
- Consider Sclerotherapy if Not Recurrent or Infected
- Consider Conservative Management with Compression and Needle Aspiration if Small (< 50 mL)
References
- De Coninck T, Vanhoenacker F, Verstraete K. Imaging Features of Morel-Lavallée Lesions. J Belg Soc Radiol. 2017 Dec 16;101(Suppl 2):15. (License: CC BY-4.0)
- Rha EY, Kim DH, Kwon H, Jung SN. Morel-lavallee lesion in children. World J Emerg Surg. 2013 Dec 30;8(1):60. (License: CC BY-2.0)
- Kontis E, Vezakis A, Psychogiou V, Kalogeropoulos P, Polydorou A, Fragulidis G. Morel-lavallée lesion: report of a case of unknown mechanism. Case Rep Surg. 2015;2015:947450. (License: CC BY-3.0)

