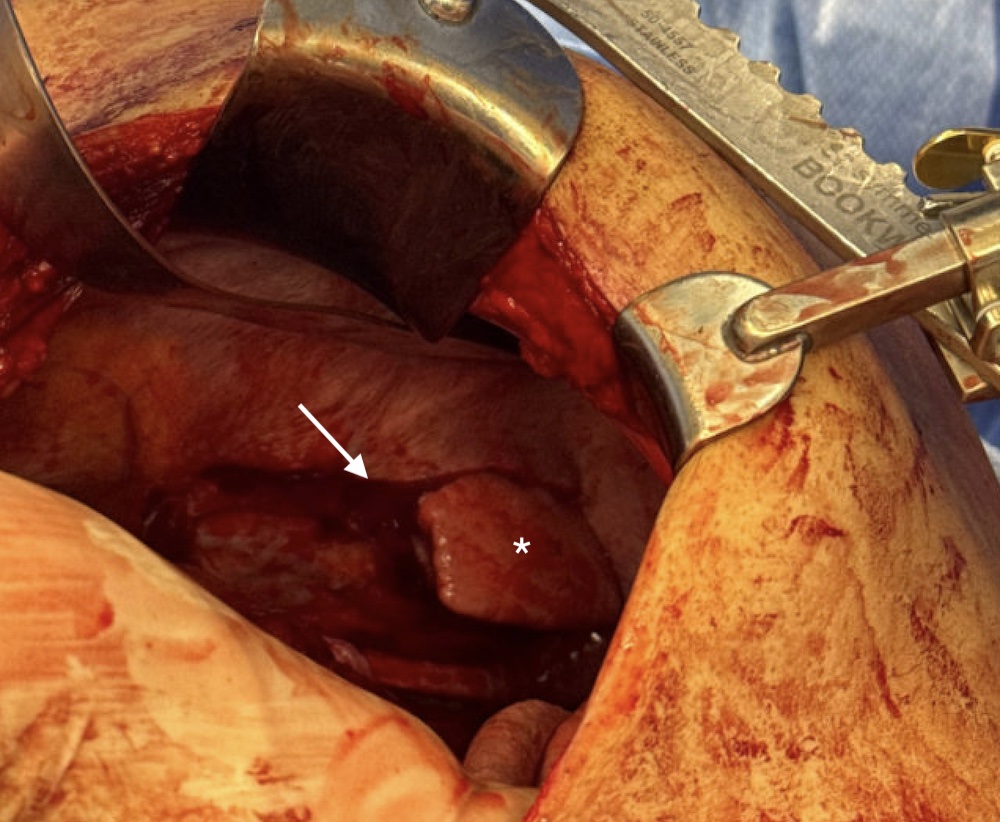
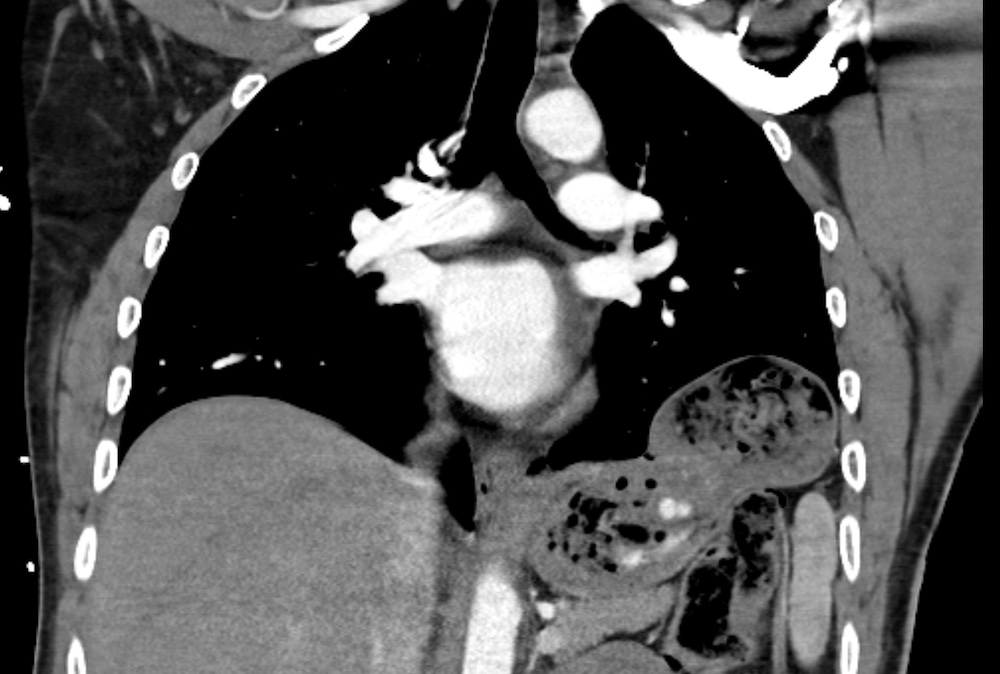
Diaphragm Injury Diaphragm Injury David Ray Velez, MD Table of Contents GeneralDiagnosisTreatment General Definition: Injury of the DiaphragmMost Common After Blunt TraumaSiteMost Common on the LeftMost Common in the Posterolateral Aspect of the Hemidiaphragm Between the Lumbar and Intercostal Muscle Slips (Weakest Point)Most Common Herniated Organs: Stomach and ColonComplicationsRespiratory FailureStrangulation of Herniated ContentsBowel ObstructionGastric VolvulusTension GastrothoraxAAST Diaphragm Injury Scale*See AASTInjury Scale is Under CopyrightTypical Severity by MechanismStabs and Low-Velocity GSW: Grade I-IIBlunt Trauma: Grade III-IVHigh-Velocity GSW, Shotgun, or Explosion: Grade V Diaphragm Laceration (Arrow) and Herniated Lung (Asterisk) Diagnosis Diagnosis Can Be Made Intraoperatively or RadiographicallySensitivityPlain Radiograph: Low Sensitivity (17-62% Sensitivity)CT: Best Imaging Modality (56-87% Sensitivity with 75-100% Specificity)eFAST/POCUS: Can Detect Signs but Highly Operator DependentRadiographic SignsUnable to Trace the Normal Diaphragm ContourElevated HemidiaphragmHerniated Abdominal Organs (Gastric Bubble in the Chest)Mediastinal ShiftNG Tube Above the DiaphragmCollar Sign (Hourglass Sign): Waist-Like Constriction of Herniated Viscera at the Level of the DiaphragmCottage Loaf Sign: Collar Sign Involving the Liver Herniating Through a Right Diaphragm Defect, Similar Appearance to a Cottage LoafDependent Viscera Sign: When Lying Supine, Herniated Organs Fall Against the Posterior Ribs Due to Loss of Diaphragm SupportIndirect Signs:HemothoraxHemoperitoneumAssociated Rib FractureAssociated Pulmonary Contusion Traumatic Diaphragmatic Hernia on CXR Collar Sign on CT Treatment TreatmentContusion (Grade I): ConservativeLaceration (Grade II-V): Surgical RepairSurgical RepairGenerally Repaired PrimarilyClassically Described Using Permanent Sutures (Prolene) in Horizontal Mattress FashionUse Mesh if Large or Under TensionUse Permanent MeshConsider Incision of Peripheral Attachments and Reattachment 2-3 Interspaces More Cephalad if NecessaryReattach Diaphragm to Ribs if Completely AvulsedPlace Sutures Circumferentially Around the RibsMay Also Consider Using Rib Suture AnchorsSurgical Timing/ApproachEarly Diagnosis (< 1 Week): Transabdominal ApproachDelayed Diagnosis (> 1 Week): Transthoracic ApproachTo Evaluate Viscera and Adhesions