Cricothyroidotomy
Cricothyroidotomy
David Ray Velez, MD
Table of Contents
General Considerations
Definition: An Emergent Surgical Airway Through an Incision in the Cricothyroid Membrane
Also Known as “Cricothyrotomy” or “Cric”
Use
- Cricothyroidotomy is the Most Rapid Surgical Approach to Secure the Airway
- Formal Tracheostomy is Too Slow for the Emergent Setting
- Cricothyroidotomy is Too Superior in the Neck to Allow Long-Term Airway Control – High Risk for Tracheal Stenosis
- Used as a Temporary Measure Until a Formal Tracheostomy Can Be Performed in a Controlled Setting
- Generally Prefer to Formalize within 24 Hours to Avoid Complications
Indications
- Cricothyroidotomy is Indicated Emergently if Unable to Intubate or Ventilate
- Many Follow a “Three-Strikes” Rule: If Unable to Secure Endotracheal Intubation After Three Attempts by the Most-Competent Provider, Secure the Airway Through Cricothyroidotomy
- Common Causes:
- Maxillofacial Trauma
- Neck Trauma
- Severe Inhalational Injury with Airway Edema
- Anaphylaxis
- Facial/Oropharyngeal Swelling/Edema
- Airway Obstruction by Foreign Body (Food/Teeth)
- Congenital Deformity
Contraindications
- The Only Contraindication is Young Age (< 10-12 Years Old)
- The Cricothyroid Membrane is Too Delicate
- Needle Cricothyroidotomy if a Surgical Airway Required
- *See Needle Cricothyroidotomy
Equipment
- Minimum Equipment:
- Scalpel
- Finger
- Tracheostomy or Endotracheal Tube (6.0 mm Generally Preferred)
- Additional Equipment:
- Bougie
- Trousseau Dilator
- Surgical Hook
Sterile Preparation May Not Be Possible in a True Emergency
There Will Be Significant Bleeding – Ignore Initially and Secure the Airway Before Managing Bleeding
Indicators of Difficult Cricothyroidotomy: SHORT Mnemonic
- Surgery
- Hematoma or Abscess
- Obesity
- Radiation Distortion or Deformity
- Tumor
Complications
- Failure to Achieve Access
- Death
- Bleeding
- Infection
- Pneumothorax
- Laryngeal Injury
- Cartilage Fracture (Thyroid or Cricoid Cartilage)
- Can Cause Vocal Cord Dysfunction/Paralysis After Decannulation
- Esophageal Injury and Tracheoesophageal Fistula
- Tracheal Stenosis
Standard Technique
Palpate and Identify Anatomical Landmarks
- Thyroid Cartilage
- Cricoid Cartilage
- Cricothyroid Membrane
Skin Incision (Vertical)
- Vertical Midline Incision is Generally Preferred to Limit Bleeding
- Some Prefer Horizontal Incisions
- Length: 3-5 cm
- Use Hands to Stabilize the Trachea if Able
Palpate and Incise the Cricothyroid Membrane (Horizontal)
- Between the Thyroid and Cricoid Cartilages
- May Require Some Dissection to Identify if Deep (Obese, Short Neck, Swelling)
Access the Trachea
- Options:
- Finger
- Trousseau Dilator
- Bougie
- Back of a Scalpel – Take Extreme Caution Not to Cut Yourself in the Moment
- Can Consider Placing Bougie Along a Finger into the Trachea to Guide the Tracheostomy Tube
Insert Tracheostomy Tube
- Generally Use a 6.0 mm Tube
- Can Insert a Regular Endotracheal Tube if a Tracheostomy Tube is Not Immediately Available
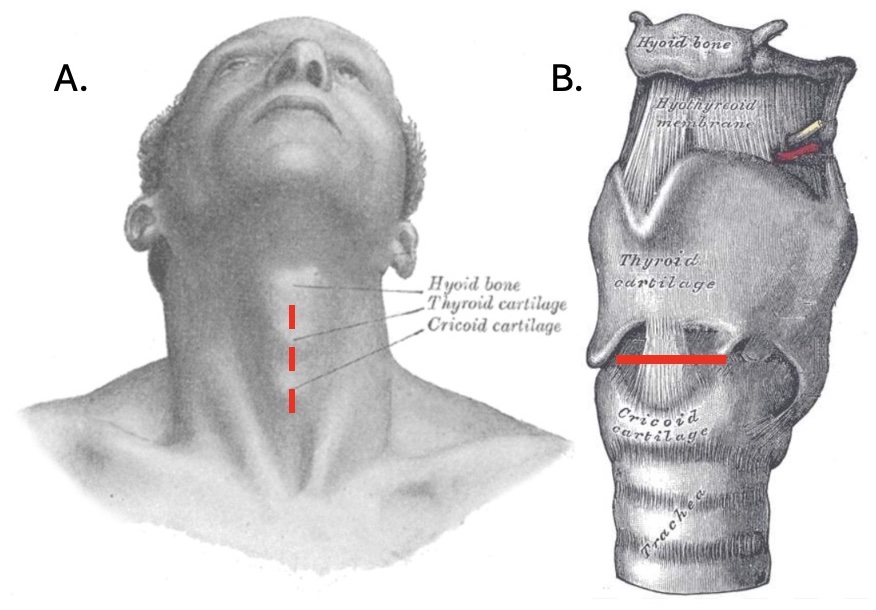
Cricothyroidotomy: (A) Vertical Skin Incision, (B) Horizontal Incision Through the Cricothyroid Membrane
Rapid Four-Step Technique (RFST)
Step 1: Palpate the Cricothyroid Membrane
Step 2: Stab Incision Through Both the Skin and Cricothyroid Membrane
Step 3: Use Hook to Retract the Larynx Caudally
Step 4: Insert the Tracheostomy Tube
Percutaneous (Seldinger) Technique
Uses a Modified Seldinger Approach Via Needle and Guidewire
Palpate and Identify Anatomical Landmarks
- Thyroid Cartilage
- Cricoid Cartilage
- Cricothyroid Membrane
Needle
- Use a Hollow Introducer Needle to Puncture Through the Skin and Cricothyroid Membrane into the Trachea
- Applying Negative Pressure to the Syringe While Placing, Bubbles Indicate Tracheal Access
Guidewire
- Pass a Guidewire Through the Needle
- Withdraw the Needle Over the Guidewire, Leaving the Guidewire in the Trachea
- Always Maintain Control of the Guidewire During Placement
Dilate the Tract
- Make a Small Skin Incision at the Entry Site
- Pass a Dilator Over the Guidewire to Dilate the Tract
Place the Tracheostomy Tube
- Pass the Tracheostomy Tube Over the Guidewire
- Withdraw the Guidewire
- Begin Ventilating Through the Tracheostomy Tube