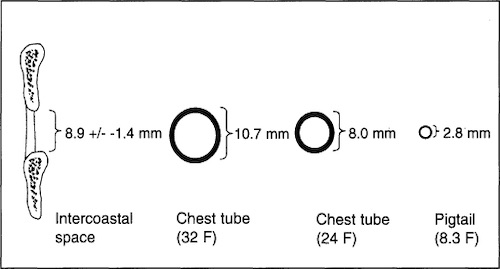
Chest Tube Sizes Compared to Average Intercostal Space (Mid-Axillary 5th Space) 1
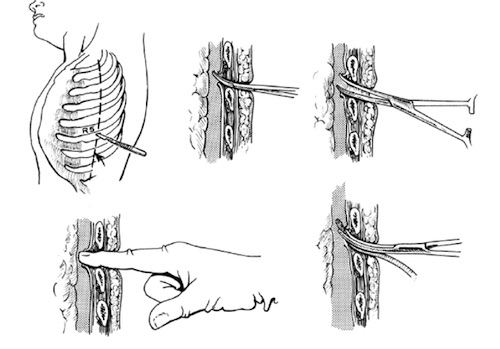
Chest Tube Placement 2
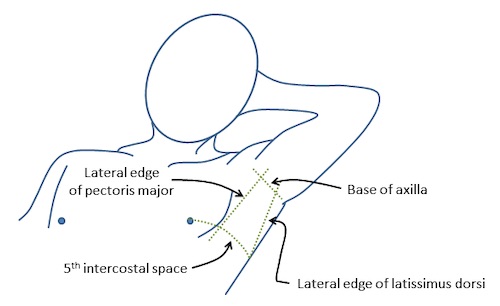
Triangle of Safety 3

Classic “Three Bottle” System 4
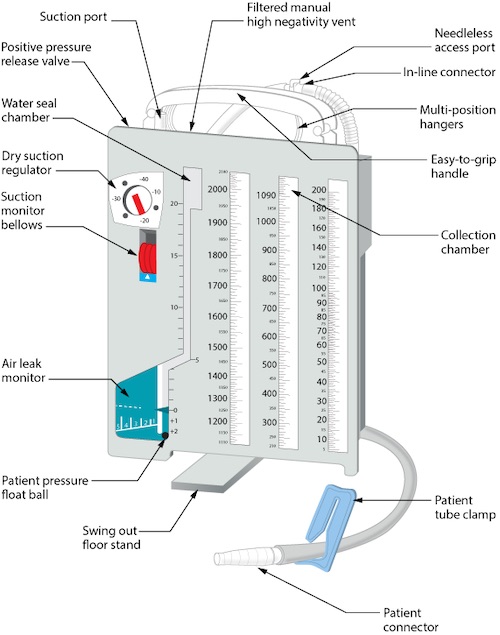
Modern Collecting System 5
Chest Tube Sizes Compared to Average Intercostal Space (Mid-Axillary 5th Space) 1
Chest Tube Placement 2
Triangle of Safety 3
Classic “Three Bottle” System 4
Modern Collecting System 5

