Consider Primary Repair if There is No Loss of Length or Significant Narrowing
Distal Injury: Ligation
Cardiorrhaphy with Pledgets 2
References
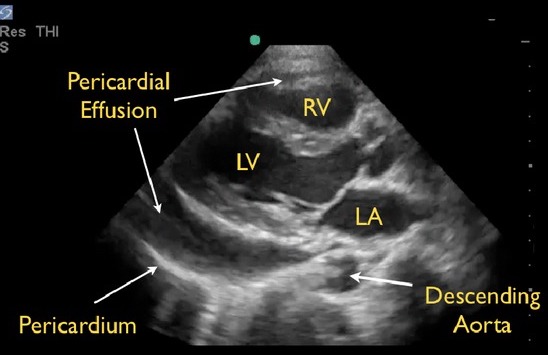
Seif D, Perera P, Mailhot T, Riley D, Mandavia D. Bedside ultrasound in resuscitation and the rapid ultrasound in shock protocol. Crit Care Res Pract. 2012;2012:503254. (License: CC BY-3.0)
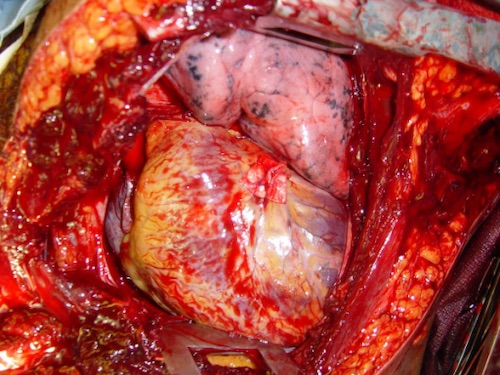
Cothren CC, Moore EE. Emergency department thoracotomy for the critically injured patient: Objectives, indications, and outcomes. World J Emerg Surg. 2006 Mar 24;1:4. (License: CC BY-2.0)