
Vancouver Classification of BTAI 1
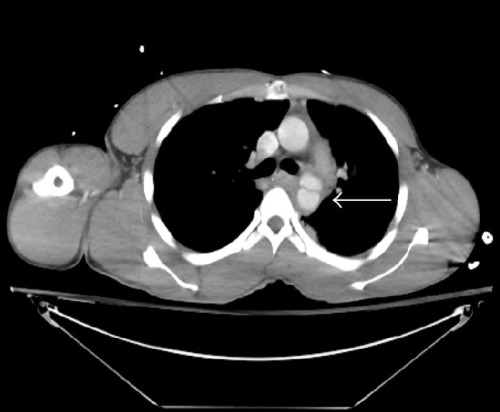
Grade III BTAI – Pseudoaneurysm 2
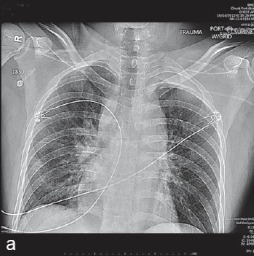
BTAI on CXR (Indistinct Aortic Knob and Widened Mediastinum 3
Vancouver Classification of BTAI 1
Grade III BTAI – Pseudoaneurysm 2
BTAI on CXR (Indistinct Aortic Knob and Widened Mediastinum 3