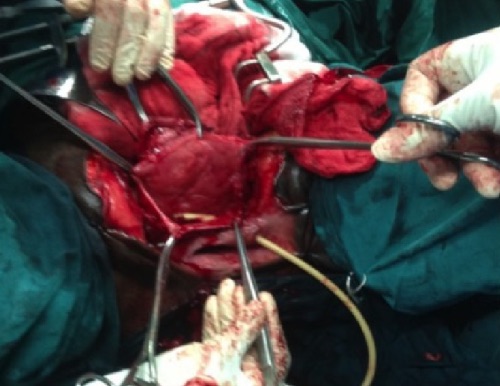
Ojewola RW, Tijani KH, Badmus OO, Oliyide AE, Osegbe CE. Extraperitoneally Ruptured, Everted, and Prolapsed Bladder: A Very Rare Complication of Pelvic Injury. Case Rep Urol. 2015;2015:476043. (License: CC BY-3.0)
Vagholkar K, Vagholkar S. Posttraumatic Haematuria with Pseudorenal Failure: A Diagnostic Lead for Intraperitoneal Bladder Rupture. Case Rep Emerg Med. 2016;2016:4521827. (License: CC BY-4.0)
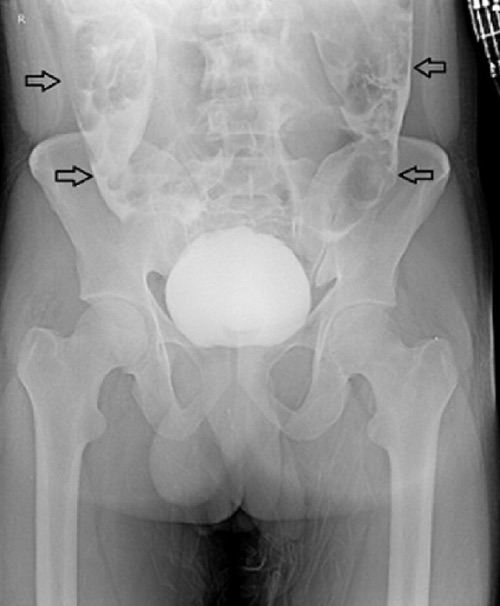
Kim JH, Ha YC, Kim TH, Myung SC, Moon YT, Kim KD, Chang IH. Delayed presentation of intravesical bone penetration after pelvic ring fracture. Korean J Urol. 2012 Dec;53(12):887-9. (License: CC BY-NC-3.0)