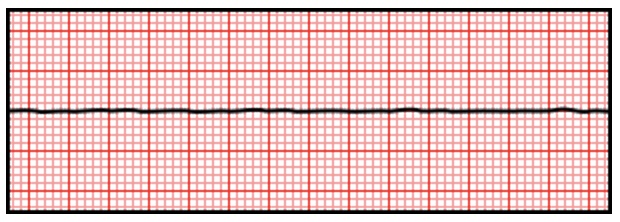
Asystole Asystole David Ray Velez, MD Cardiac Arrest with Complete Cessation of Electrical Activity in the HeartThe Terminal Rhythm/Endpoint of All Cardiac ArrestEKG PatternNo WaveformOnly an Isoelectric “Flat Line” Asystole Reversible Causes of Sudden Cardiac Arrest: “5 H’s and T’s”5 H’s:HypovolemiaHypoxiaHydrogen Ions (Acidosis)Hypokalemia/HyperkalemiaHypothermia/Hyperthermia5 T’s:Tension PneumothoraxTrauma and ToxinsTamponade (Cardiac)Thrombosis (Pulmonary/PE)Thrombosis (Coronary/MI)“H’s and T’s” are More Often are Associated with PEA Than Asystole TreatmentFollow ACLS Guidelines: *See Cardiac ArrestStart CPR Immediately and Give OxygenTreat Any Reversible CausesCheck Rhythm Every 2 MinutesAsystole is Not a Shockable RhythmEpinephrine: 1 mg IV/IO, Repeat Every 3-5 Minutes*See Antiarrhythmic PharmacologyAdjuncts:Calcium ChlorideDose: 1 g IVVasopressor and Inotropic EffectsNot Routinely Given but May Be ConsideredSodium BicarbonateDose: 50-100 mEq IV (1-2 Amps/Ampules)Can Mitigate the Effects of Acidosis and HyperkalemiaNot Routinely Given but May Be Considered if Concerned for Significant Acidosis or Hyperkalemia Cardiac Arrest Management Algorithm:Immediate CPR and OxygenCheck Rhythm Every 2 Minutes:VF/pVT:DefibrillateAlternate Epinephrine and Amiodarone After Each CheckPEA/Asystole:Epinephrine After Every Other CheckAdjuncts:Calcium ChlorideSodium Bicarbonate