Arterial Blood Gas (ABG) Analysis
Arterial Blood Gas (ABG) Analysis
David Ray Velez, MD
Table of Contents
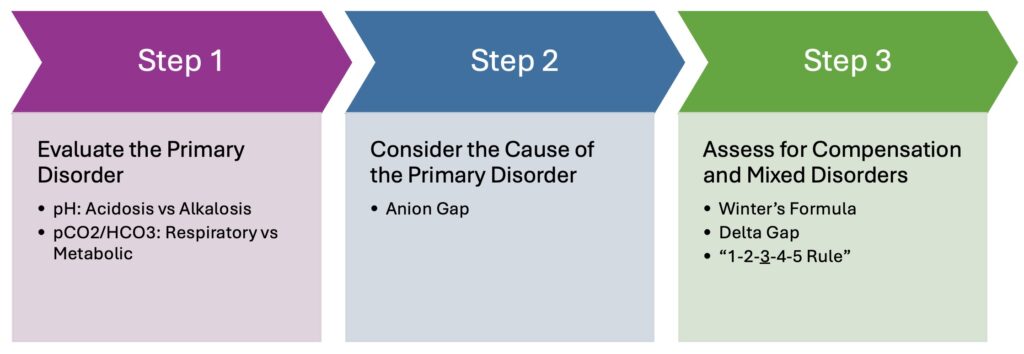
Evaluation of Primary Disorder
Normal Blood Gas Values
| Arterial (ABG) | Venous (VBG) | |
| pH | 7.40 (7.35-7.45) | 7.37 (7.32-7.42) |
| pO2 | 80-100 mmHg | 35-45 mmHg |
| pCO2 | 40 (35-45) mmHg | 46 (41-51) mmHg |
| HCO3 | 24 (22-26) mEq/L | 26 (24-28) mEq/L |
| Base Excess | 0 (-2 to +2) | 0 to +4 |
Evaluation of Simple Primary Disturbance
- pH < 7.35 = Acidosis
- pCO2 > 45 = Respiratory Acidosis
- HCO3 < 22 = Metabolic Acidosis
- pH > 7.45 = Alkalosis
- pCO2 < 35 = Respiratory Alkalosis
- HCO3 > 26 = Metabolic Alkalosis
Buffering System: H + HCO3 = H2CO3 = CO2 + H2O
Compensation
- Metabolic Disorders: Respiratory Compensation Occurs Rapidly Over Minutes-Hours (Change in Ventilation)
- Respiratory Disorders: Renal Compensation Occurs Slowly Over Days-Weeks (Change in Acid Excretion and Bicarbonate Reabsorption)
Simple vs Mixed Disorders
- Simple Acid-Base Disorder: A Single Disorder with Appropriate Respiratory or Renal Compensation
- Mixed Acid-Base Disorder: Multiple Disorders Present Simultaneously
Respiratory Acidosis
Respiratory Acid-Base Disorders are Compensated by Renal Changes in Bicarbonate Reabsorption (Slow Process Over Days-Weeks)
Acuity/Compensation
- Acute Respiratory Acidosis – High pH Changes are Seen with Minimal Compensation
- Only Slight Compensation Occurs Over Minutes-Hours from Cellular Buffering of Plasma Proteins
- Chronic Respiratory Acidosis – pH More Normalized Due to Renal Compensation Over Days-Weeks with Increased Reabsorption of Bicarbonate and Excretion of Acid
Expected Change in Bicarbonate and pH (For Every 10 mmHg Increased in pCO2 Above 40 mmHg)
- Acute Respiratory Alkalosis:
- HCO3 Increases 1 mEq/L Above 24
- pH Decreases 0.08 Below 7.40
- Chronic Respiratory Alkalosis:
- HCO3 Increases 3-4 mEq/L Above 24
- pH Decreases 0.03 Below 7.40
- Mnemonic: “1-2-3-4-5 Rule”
- Expected Change in HCO3 (mEq/L) for Every 10 mmHg Change in pCO2 Due to Respiratory Acid-Base Disorders
| Acute | Chronic | |
| Respiratory Acidosis (↑ CO2) | ↑ 1 | ↑ 4 |
| Respiratory Alkalosis (↓ CO2) | ↓ 2 | ↓ 5 |
Respiratory Alkalosis
Respiratory Acid-Base Disorders are Compensated by Renal Changes in Bicarbonate Reabsorption (Slow Process Over Days-Weeks)
Acuity/Compensation
- Acute Respiratory Alkalosis – High pH Changes are Seen with Minimal Compensation
- Chronic Respiratory Alkalosis – pH More Normalized Due to Renal Compensation Over Days-Weeks with Decreased Reabsorption of Bicarbonate
Expected Change in Bicarbonate
- Acute Respiratory Alkalosis: HCO3 = 24 – 2 x (40 – pCO2) / 10
- Chronic Respiratory Alkalosis: HCO3 = 24 – 5 x (40 – pCO2) / 10
- Mnemonic: “1-2-3-4-5 Rule”
- Expected Change in HCO3 (mEq/L) for Every 10 mmHg Change in pCO2 Due to Respiratory Acid-Base Disorders
| Acute | Chronic | |
| Respiratory Acidosis (↑ CO2) | ↑ 1 | ↑ 4 |
| Respiratory Alkalosis (↓ CO2) | ↓ 2 | ↓ 5 |
Metabolic Acidosis
Anion Gap
- Anion Gap = Na – (HCO3 + Cl)
- Gap > 12: Anion Gap Metabolic Acidosis (AGMA)
- Gap ≤ 12: Non-Anion Gap Metabolic Acidosis (Non-AGMA)
Metabolic Acidosis is Compensated by Pulmonary Changes with Increased Ventilation (Decreased CO2)
Compensation
- Winter’s Formula
- Expected pCO2 = (1.5 x HCO3) + 8 ± 2
- Used to Determine if Respiratory Compensation is Appropriate
- Other Methods to Approximate Expected pCO2
- Expected pCO2 = HCO3 + 15
- Expected pCO2 Approximates the Decimal Digits of Arterial pH (pH 7.27 with pCO2 27 mmHg)
- Interpretation:
- Actual PCO2 Within Expected Values: Adequate Respiratory Compensation
- Actual PCO2 > Expected: Secondary Respiratory Acidosis or Mixed Acid Base Disorder
- Actual PCO2 < Expected: Secondary Respiratory Alkalosis or Mixed Acid Base Disorder
Delta Gap (ΔΔ)
- Formula Used in Evaluating Anion Gap Metabolic Acidosis (AGMA) for Additional Disturbances
- Delta Gap (ΔΔ) = Change in Anion Gap – Change in Bicarb
- Change in Anion Gap = AG – 12
- Change in Bicarb = 24 – HCO3
- Gap Interpretation:
- Significantly Positive (> 6): Mixed AGMA and Metabolic Alkalosis
- Decrease in Bicarbonate is Less than Expected
- Near-Equal (-6 to +6): AGMA Alone
- Significantly Negative (< -6): Mixed AGMA and Non-AGMA
- Rise in Anion Gap is Not as Significant as the Observed Decrease in Bicarbonate
- Significantly Positive (> 6): Mixed AGMA and Metabolic Alkalosis
- Delta Ratio = Change in Anion Gap / Change in Bicarb
- Change in Anion Gap = AG – 12
- Change in Bicarb = 24 – HCO3
- Ratio Interpretation:
- < 0.4: Non-AGMA Alone
- 4-0.8: Mixed AGMA and Non-AGMA
- 8-2.0: AGMA Alone
- > 2.0: Mixed AGMA and Metabolic Alkalosis
Metabolic Alkalosis
Metabolic Alkalosis is Compensated by Pulmonary Changes with Decreased Ventilation (Increased CO2)
Expected CO2 = (0.7 x HCO3) + 20 mmHg ± 5