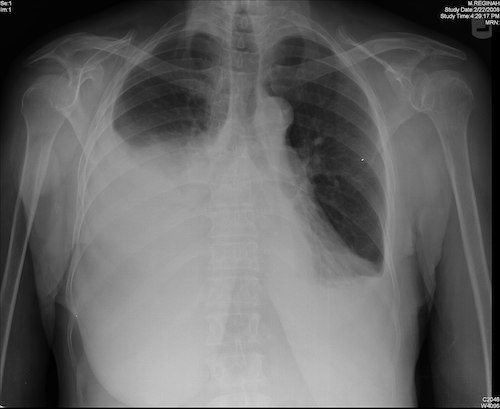
Pleural Effusion Pleural Effusion David Ray Velez, MD Table of Contents DefinitionCausesPleural Fluid PhysiologyDiagnosisTreatment Definition Pleural Effusion Definition: Fluid within the Pleural SpaceTypesTransudative Pleural Effusion: From Unbalanced Hydrostatic and Osmotic PressuresResults in Smaller ProteinsExudative Pleural Effusion: From Inflammation Increasing Capillary PermeabilityResults in Larger Proteins Causes Transudative Pleural EffusionCongestive Heart Failure (CHF) – The Most Common Transudative CauseAtelectasisHepatic HydrothoraxHypoalbuminemiaNephrotic SyndromeExudative Pleural EffusionMalignancy – The Most Common Exudative CauseHemothorax (HTX)*See Hemothorax (HTX)Parapneumonic Effusion or Empyema*See Parapneumonic Effusion and Empyema – The O.R.Chylothorax*See Chylothorax – The O.R.AmyloidosisSarcoidosisPulmonary Embolism Pleural Fluid Physiology FunctionSerous FluidActs as a Lubricant for the Parietal and Visceral PleuraPrevents Adhesion During RespirationFlowProduction: Parietal Circulation (Intercostal Arteries) from Bulk FlowReabsorption: Lymphatic SystemMostly (75%) from Lymphatics of the Parietal PleuraVisceral Pleural Plays No Significant Role in DrainageThe Parietal Pleura is the Primary Determinant of Fluid TurnoverVolumeNormal Volume: 10-20 ccFluid Turnover Ability: 1-2 L/DayCan Increase Up to 40x Normal RatesRequires a Profound Increase in Production or Blockage of Lymphatics to Initiate Fluid Accumulation Diagnosis Generally a Radiographic Diagnosis (CXR, CT, or POCUS)Minimum Volume Required to Be Seen on a Standard Upright PA CXR: 300 ccDifferential EvaluationThoracentesis and Pleural Fluid EvaluationRoutine Orders:Cell Count/DifferentialpHProtein (Pleural and Serum)LDH (Pleural and Serum)Also Consider:GlucoseAmylaseCholesterolTriglyceridesBacterial CultureLight’s CriteriaIndicates that the Effusion is ExudativeCriteria (Requires ≥ One):Pleural:Serum Protein Ratio > 0.5Pleural:Serum LDH > 0.6Pleural LDH > 2/3 the Upper Limit of NormalThree-Test RuleIndicates that the Effusion is ExudativeCriteria (Requires ≥ One):Pleural Protein > 2.9 g/dLPleural Cholesterol > 45 mg/dLPleural LDH > 0.45x the Upper Limit of Normal Transudate Exudate WBC < 1,000 > 1,000 pH 7.40-7.55 7.30-7.45 Pleural:Serum Protein Ratio < 0.5 > 0.5 Pleural:Serum LDH Ratio < 0.6 > 0.6 Cholesterol < 45 mg/dL > 45 mg/dL Specific MeasuresComplicated Parapneumonic Effusion/Empyema: WBC > 50,000 and pH < 7.30Chylothorax: Triglycerides > 110 mg/dL Pleural Effusion 1 Treatment Treat Any Underlying DisorderFluid DrainageAsymptomatic: Generally No Drainage RequiredSymptomatic: Thoracentesis vs. Thoracostomy Tube (Chest Tube)*See Thoracostomy Tube (Chest Tube)Thoracentesis Improves Oxygenation but No Significant Effect on A-a Gradient, LOS, or MortalityStop Immediate Drainage if Having Pain or Total Fluid > 1.0-1.5 LAt Risk for Re-Expansion Pulmonary Edema When Larger Volumes are DrainedIf Fails: Thoracoscopic Talc Pleurodesis vs Long-Term DrainageMalignant Pleural Effusion (MPE): Indications for a Tunneled Pleural CatheterRecurrent Symptomatic Fluid Build-UpShort Life-Expectancy (< 3 Months)Poor Functional StatusTrapped LungBulky Pleural MetastasesFailed PleurodesisPatient Preference Over Repeated Thoracentesis or Surgical Intervention References Rosen Y. Wikimedia Commons. (License: CC BY-SA-2.0)